

Hemodynamic rounds: Dilemma in the management of disconnected pulmonary arteries with double arterial ducts
- PMID: 35847398
- PMCID: PMC9280097
- DOI: 10.4103/apc.apc_75_21
Hemodynamic rounds: Dilemma in the management of disconnected pulmonary arteries with double arterial ducts
Abstract
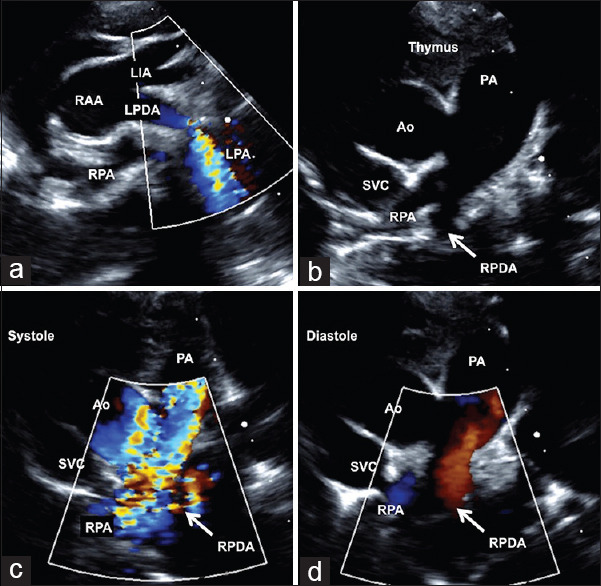
Segmental pulmonary arterial hypertension occurs when the right and left pulmonary arteries are nonconfluent and receive blood supply from different sources. High blood pressure confined to limited lung segments may accelerate progression of pulmonary vascular resistance. Calculation of segmental vascular resistance and assessment of operability in such situations are done after integrating catheter hemodynamics, magnetic resonance imaging techniques, or perfusion scintigraphy. When an isolated pulmonary artery perfused by a restrictive ipsilateral arterial duct is associated with a large nonrestrictive contralateral arterial duct connected to the other pulmonary artery, leading to unilateral pulmonary arterial hypertension and features of high vascular resistance, it offers unique challenges to decision-making.
Keywords: Differential lung perfusion; double patent arterial ducts; isolation of pulmonary artery; pulmonary vascular resistance; segmental pulmonary hypertension.
Copyright: © 2021 Annals of Pediatric Cardiology.
Conflict of interest statement
There are no conflicts of interest.
Figures




Comment in
-
Re; Dilemma in the management of disconnected pulmonary arteries with double arterial ducts.Ann Pediatr Cardiol. 2022 Jul-Aug;15(4):437. doi: 10.4103/apc.apc_72_22. Epub 2023 Jan 6. Ann Pediatr Cardiol. 2022. PMID: 36935833 Free PMC article. No abstract available.
References
-
- Ten Harkel AD, Blom NA, Ottenkamp J. Isolated unilateral absence of a pulmonary artery: A case report and review of the literature. Chest. 2002;122:1471–7. - PubMed
-
- Batlivala SP, McElhinney DB, Pigula FA, Marshall AC. Isolated pulmonary artery arising from a duct: A single-center review of diagnostic and therapeutic strategies. J Thorac Cardiovasc Surg. 2014;148:2245–52. - PubMed
-
- Santoro G, Caianiello G, Russo MG, Calabrò R. Stenting of bilateral arterial ducts in complex congenital heart disease. Pediatr Cardiol. 2008;29:842–5. - PubMed
-
- Viswanathan S, Kumar RK. Assessment of operability of congenital cardiac shunts with increased pulmonary vascular resistance. Catheter Cardiovasc Interv. 2008;71:665–70. - PubMed
-
- Kellenberger CJ, Macgowan CK, Roman KS, Al-Habshan F, Benson LN, Redington AN, et al. Hemodynamic evaluation of the peripheral pulmonary circulation by cine phase-contrast magnetic resonance imaging. J Magn Reson Imaging. 2005;22:780–7. - PubMed
Publication types
LinkOut - more resources
Full Text Sources