

The relationship between the gut microbiome and the risk of respiratory infections among newborns
- PMID: 35847562
- PMCID: PMC9283516
- DOI: 10.1038/s43856-022-00152-1
The relationship between the gut microbiome and the risk of respiratory infections among newborns
Abstract
Background: Emerging evidence points to a critical role of the developing gut microbiome in immune maturation and infant health; however, prospective studies are lacking.
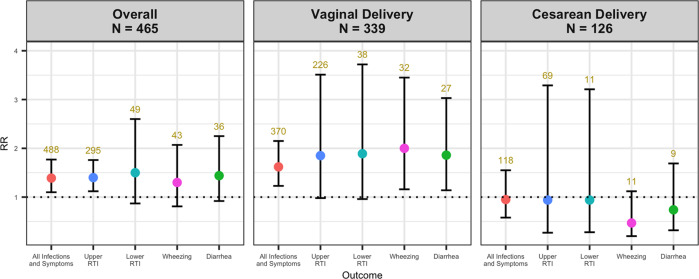
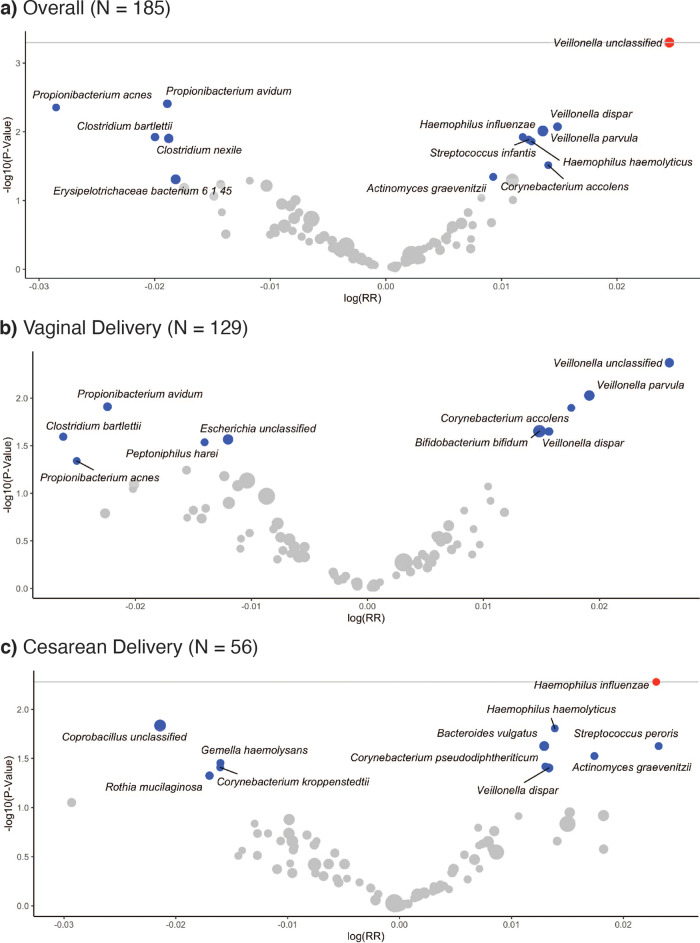
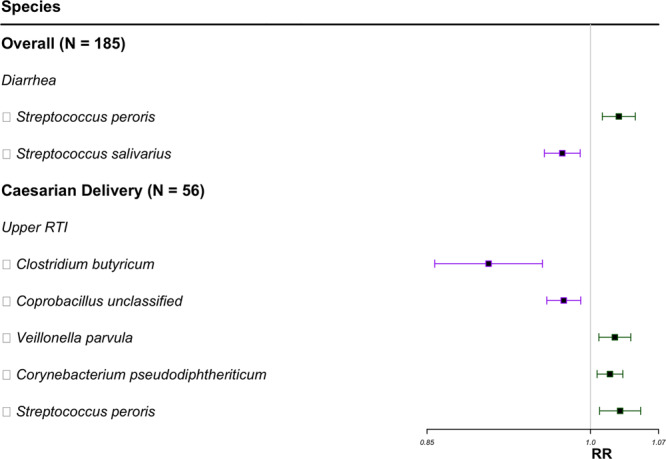
Methods: We examined the occurrence of infections and associated symptoms during the first year of life in relation to the infant gut microbiome at six weeks of age using bacterial 16S rRNA V4-V5 gene sequencing (N = 465) and shotgun metagenomics (N = 185). We used generalized estimating equations to assess the associations between longitudinal outcomes and 16S alpha diversity and metagenomics species.
Results: Here we show higher infant gut microbiota alpha diversity was associated with an increased risk of infections or respiratory symptoms treated with a prescription medicine, and specifically upper respiratory tract infections. Among vaginally delivered infants, a higher alpha diversity was associated with an increased risk of all-cause wheezing treated with a prescription medicine and diarrhea involving a visit to a health care provider. Positive associations were specifically observed with Veillonella species among all deliveries and Haemophilus influenzae among cesarean-delivered infants.
Conclusion: Our findings suggest that intestinal microbial diversity and the relative abundance of key taxa in early infancy may influence susceptibility to respiratory infection, wheezing, and diarrhea.
Keywords: Biomarkers; Epidemiology; Microbiome; Paediatric research.
© The Author(s) 2022.
Conflict of interest statement
Competing interestsThe authors declare no competing interests.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
