

En Bloc Resection of Right Renal Cell Carcinoma and Inferior Vena Cava Tumor Thrombus Without Caval Reconstruction: Is It Safe to Divide the Left Renal Vein?
- PMID: 35847837
- PMCID: PMC9280635
- DOI: 10.3389/fonc.2022.877310
En Bloc Resection of Right Renal Cell Carcinoma and Inferior Vena Cava Tumor Thrombus Without Caval Reconstruction: Is It Safe to Divide the Left Renal Vein?
Abstract
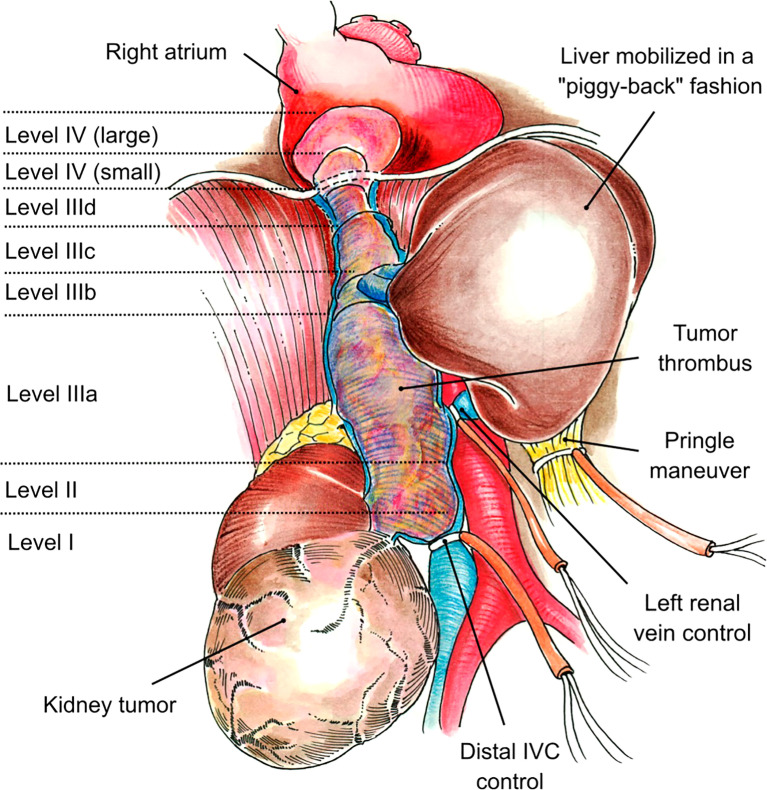
Introduction: It has been suggested that inferior vena cava (IVC) reconstruction following resection of retroperitoneal tumors with IVC tumor thrombus (TT) is not required when adequate collateral circulation is present. There are no reports evaluating mid-term effects on renal function in these patients. The purpose of this study was to assess renal function after en bloc resection of right renal cell carcinoma (RCC) with obstructing IVC TT and the possible risks that may arise after left renal vein division.
Materials and methods: A bi-institutional retrospective review was performed over a 15-year period, assessing patients with right RCC and obstructing level II-IV TT. All patients underwent extensive evaluation and cardiology clearance, and informed consent was obtained for right radical nephrectomy and thrombectomy with or without IVC reconstruction with possible cardiopulmonary bypass (CPB). Patient demographics, tumor characteristics, intraoperative factors, complications, length of stay, and patient survival were evaluated. Preoperative creatinine was recorded, as was creatinine on the day of discharge and at 6 and 12 months postoperatively.
Results: Twenty-two patients were included in the study. Median age at surgery was 62.5 (range: 45-79) years, and 19 (86%) of the patients were men. One patient (5%) had a level II thrombus, 14 patients (64%) had a level III thrombus (IIIa, n = 3; IIIb, n = 6; IIIc, n = 3; IIId, n = 2), and seven patients (32%) had a level IV thrombus. Intraoperatively, median estimated blood loss was 1.35 (range: 0.2-25) L. The median length of hospital stay was 11 (range: 5-50) days. Median preoperative creatinine was 1.20 (range: 0.40-2.70) mg/dl, and postoperatively, median creatinine was 1.3 (range: 0.86-2.20) mg/dl. Median creatinine levels at 6 months and 12 months postoperatively were 1.10 (range: 0.5-1.8) mg/dl and 1.40 (range: 0.6-2.0) mg/dl, respectively. Four patients died (range: 0.1-1.3 years), and median postoperative follow-up among the 18 ongoing survivors (at last follow-up) was 1.5 (range: 0.5-7.0) years.
Conclusions: Resection of right RCC with an obstructing level II-IV TT without reconstruction of the IVC appears to not have a significant adverse effect on mid-term renal function after division of the left renal vein.
Keywords: inferior vena cava thrombectomy; nephrectomy; oncology; renal cell carcinoma; tumor thrombus extending to inferior vena cava.
Copyright © 2022 Horodyski, Gonzalez, Tabbara, Gaynor, Rodriguez-Cabero, Herranz-Amo, Hernández, Shah and Ciancio.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



Similar articles
-
Initial Series of Robotic Segmental Inferior Vena Cava Resection in Left Renal Cell Carcinoma With Caval Tumor Thrombus.Urology. 2020 Aug;142:125-132. doi: 10.1016/j.urology.2020.03.053. Epub 2020 Apr 24. Urology. 2020. PMID: 32339559
-
[Outcome of Resection of Inferior Vena Cava Superior to the Renal Vein in Renal Cell Carcinoma with Vena Caval Tumor Thrombus].Hinyokika Kiyo. 2016 Jun;62(6):287-94. Hinyokika Kiyo. 2016. PMID: 27452491 Japanese.
-
Laparoscopic Radical Nephrectomy and Inferior Vena Cava Thrombectomy in the Treatment of Renal Cell Carcinoma.Eur Urol. 2015 Jul;68(1):115-22. doi: 10.1016/j.eururo.2014.12.011. Epub 2014 Dec 19. Eur Urol. 2015. PMID: 25534934
-
The perioperative management of an inferior vena caval tumor thrombus in patients with renal cell carcinoma.Urol Oncol. 2013 Jul;31(5):517-21. doi: 10.1016/j.urolonc.2011.03.006. Epub 2011 Apr 21. Urol Oncol. 2013. PMID: 21514183 Review.
-
Transitional cell carcinoma with extension of the renal vein and IVC tumor thrombus: report of three cases and literature review.World J Surg Oncol. 2016 Dec 28;14(1):309. doi: 10.1186/s12957-016-1041-z. World J Surg Oncol. 2016. PMID: 28031042 Free PMC article. Review.
Cited by
-
Inferior Vena Cava (IVC) Resections without Reconstruction in Renal Tumors: Two Case Reports.Diagnostics (Basel). 2023 May 16;13(10):1759. doi: 10.3390/diagnostics13101759. Diagnostics (Basel). 2023. PMID: 37238242 Free PMC article.
-
Impact of Left Renal Vein Ligation on Renal Function Following En Bloc Resection of Segmental Inferior Vena Cava and Right Kidney.Ann Surg Oncol. 2024 Jul;31(7):4787-4794. doi: 10.1245/s10434-024-15324-7. Epub 2024 May 10. Ann Surg Oncol. 2024. PMID: 38727768
-
Renal cell carcinoma with an "uncoiling" tumor thrombus: intraoperative shift from level III to level IV.World J Surg Oncol. 2024 Mar 7;22(1):76. doi: 10.1186/s12957-024-03355-z. World J Surg Oncol. 2024. PMID: 38454471 Free PMC article.
-
ASO Author Reflections: The Impact of Left Renal Vein Dissection on Renal Function in a Solitary Kidney.Ann Surg Oncol. 2024 Aug;31(8):5473-5474. doi: 10.1245/s10434-024-15389-4. Epub 2024 May 4. Ann Surg Oncol. 2024. PMID: 38704504 No abstract available.
References
-
- Gonzalez J, Gaynor JJ, Martínez-Salamanca JI, Capitanio U, Tilki D, Carballido JA, et al. . Association of an Organ Transplant-Based Approach With a Dramatic Reduction in Postoperative Complications Following Radical Nephrectomy and Tumor Thrombectomy in Renal Cell Carcinoma. Eur J Surg Oncol (2019) 45(10):1983–92. doi: 10.1016/j.ejso.2019.05.009 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials