

Home Medication Regimens Increase in Complexity After Admission for Fall in the Older Trauma Patient
- PMID: 35848087
- PMCID: PMC10829064
- DOI: 10.1177/00031348221083958
Home Medication Regimens Increase in Complexity After Admission for Fall in the Older Trauma Patient
Abstract
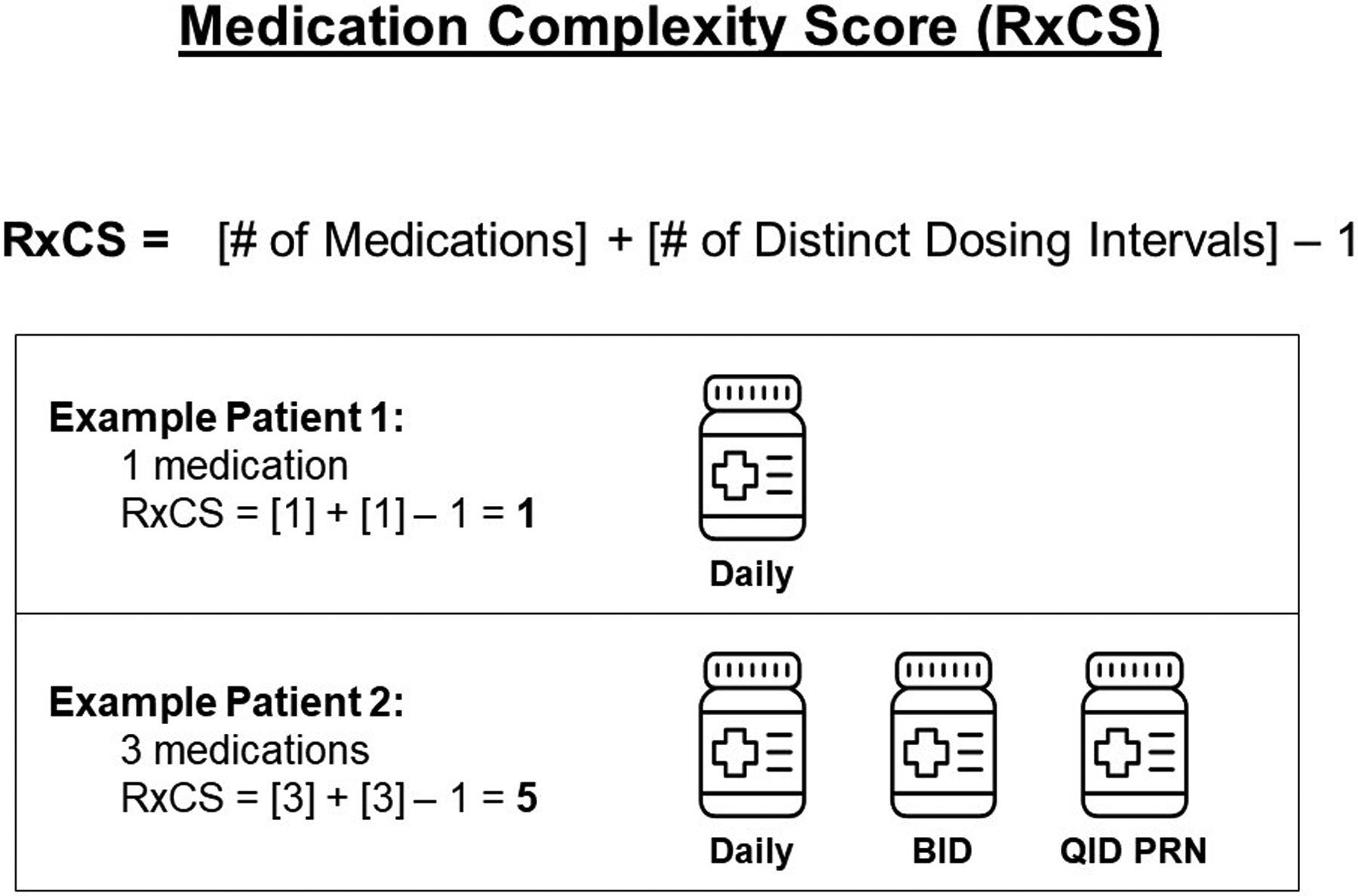
Background: Hospitalization for the older trauma patient is an opportunity to assess polypharmacy. We hypothesized that medication regimen complexity (RxCS) and pain medication prescriptions (PRxs) would increase in older home-going patients admitted for a fall.
Methods: We retrospectively chart reviewed patients ≥45 years old admitted for a fall at a level 1 trauma center who were discharged home with full medication documentation. RxCS was compared pre-admission and post-discharge with Wilcoxon signed-rank tests; opioid and non-opioid PRxs were compared with Fisher's exact test, α = .05.
Results: 103 patients met inclusion criteria; 58% were ≥65 years old. RxCS (9 [.5-13] to 11 [4.5-15], P < .01) increased on discharge. Opioid PRx rates increased significantly in all age groups. Non-opioid PRx rates increased significantly for patients <65 but not for patients ≥65.
Conclusions: Admission for a fall was associated with increases in RxCS, while PRx changes were age-dependent. Providers should recognize that admissions for older patients who fall after trauma are underutilized opportunities to address polypharmacy in high-risk patients.
Keywords: geriatrics; polypharmacy, trauma acute care; trauma.
Conflict of interest statement
Declaration of Conflicting InterestsThe author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Ho spouse is a consultant for Medtronic, Zimmer Biomet, Atricure, and Astra Zeneca. The remaining authors have no conflicts of interest to disclose.
Figures

References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
