

[Comparison of the effectiveness of the long head of the biceps tendon with or without proximal amputation after arthroscopic repair of the rotator cuff]
- PMID: 35848181
- PMCID: PMC9288905
- DOI: 10.7507/1002-1892.202203056
[Comparison of the effectiveness of the long head of the biceps tendon with or without proximal amputation after arthroscopic repair of the rotator cuff]
Abstract
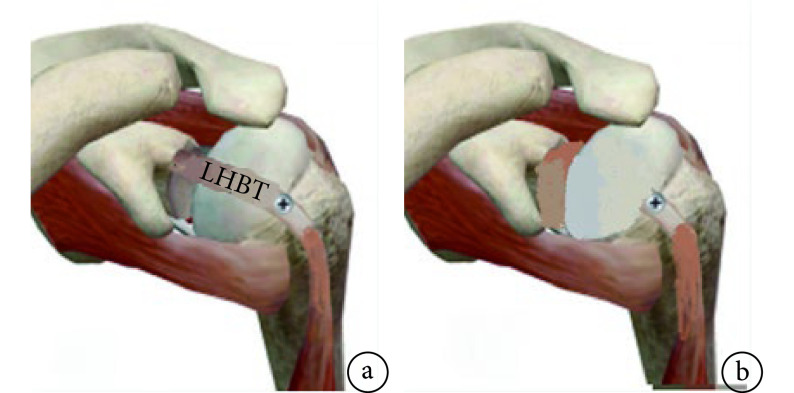
Objective: To compare the effectiveness of the long head of the biceps tendon (LHBT) with or without proximal amputation after arthroscopic rotator cuff repair in the treatment of repairable rotator cuff tear with LHBT injury.
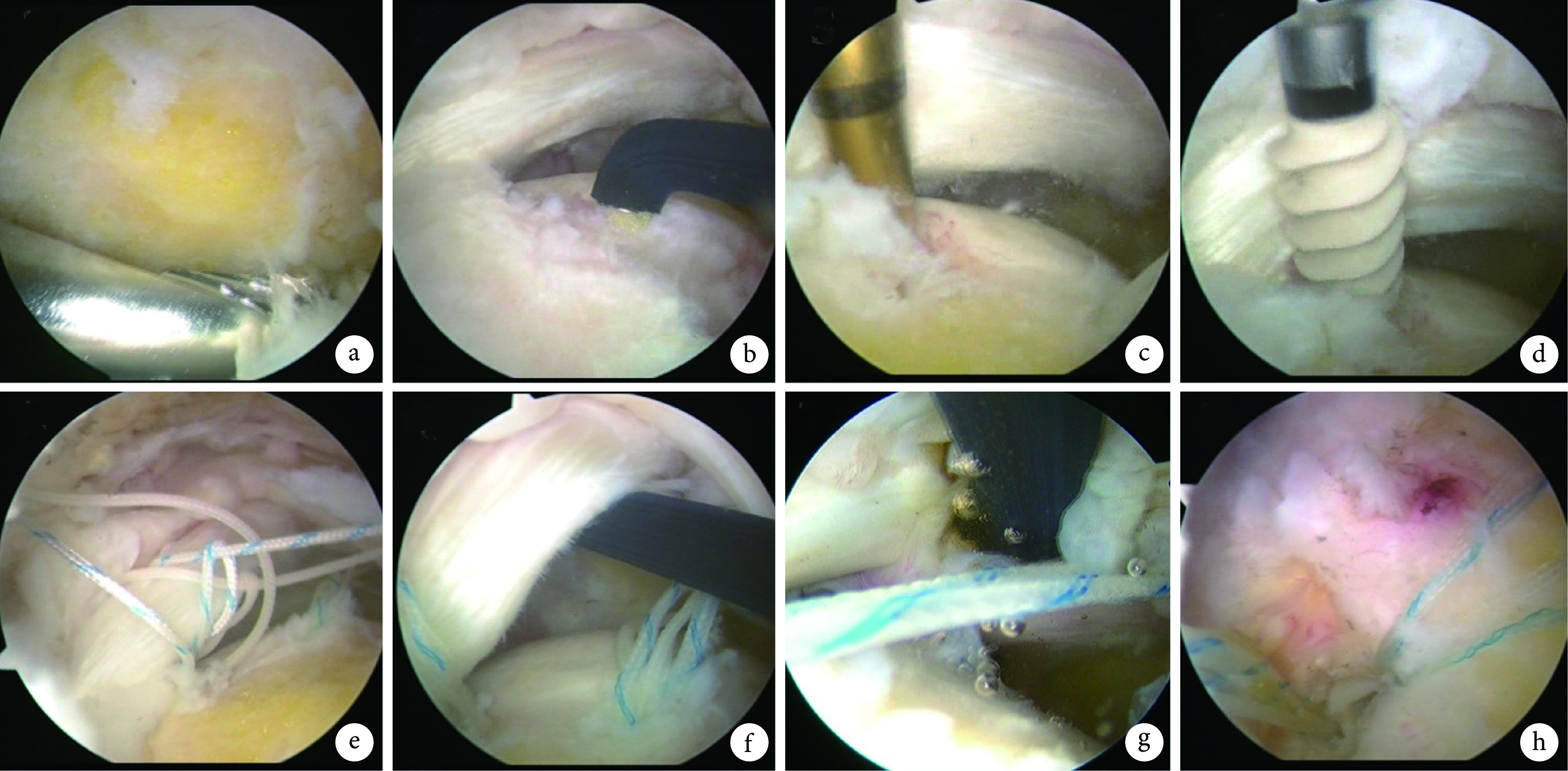
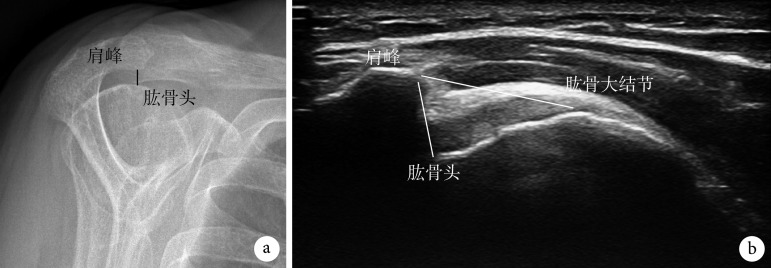
Methods: The clinical data of 68 patients with LHBT injury combined with supraspinatus tendon tear who met the selection criteria between January 2016 and June 2020 were retrospectively analyzed. According to whether the proximal end of LHBT was cut off or not after arthroscopic rotator cuff repair, they were divided into LHBT fixation without cutting group (group A, 32 cases) and LHBT fixation with cutting group (group B, 36 cases). There was no significant difference in gender, age, operating side, preoperative supraspinatus tear width, Constant-Murley shoulder function scale, University of California Los Angeles (UCLA) score, and visual analogue scale (VAS) score between the two groups ( P>0.05). The operation time, elbow flexion muscle strength, and postoperative complications were compared between the two groups. The Constant-Murley shoulder function scale, UCLA score, and VAS score were used to evaluate the recovery of shoulder function before operation and at 3, 6, 12 months after operation. The acromion-humeral distance (AHD) was measured by Y-view X-ray film of the shoulder joint immediately after operation and at last follow-up. AHD and acromion-greater tubercle distance (AGT) were measured by musculoskeletal ultrasound at 0°, 30°, 60°, and 90° of abduction.
Results: There was no significant difference in operation time between the two groups ( t=-0.740, P=0.463). Patients in both groups were followed up (13.0±0.7) months in group A and (13.1±0.8) months in group B, with no significant difference ( t=0.127, P=0.899). At last follow-up, the elbow flexor muscle strength of the two groups reached grade Ⅴ. Complications (including shoulder pain, deltoid atrophy, and rotator cuff re-tear) occurred in 6 patients (18.75%) in group A and 9 patients (25.00%) in group B, without neurovascular injury, surgical site infection, joint stiffness, LHBT spasmodic pain, and Popeye deformity. There was no significant difference in the incidence of complications between the two groups ( χ 2=0.385, P=0.535). The Constant-Murley shoulder function scale, UCLA score, and VAS score significantly improved in both groups at 3, 6, and 12 months after operation ( P>0.05). The above scores in group B were significantly better than those in group A at 3 and 6 months after operation ( P<0.05), and there was no significant difference between the two groups at 12 months after operation ( P>0.05). Y-view X-ray film measurement of the shoulder joint showed that the AHD of the two groups at last follow-up was less than that at immediate after operation, but the difference was not significant ( Z=-1.247, P=0.212); the AHD of group A was significantly greater than that of group B at last follow-up ( t=-2.291, P=0.025). During musculoskeletal ultrasound detection of abduction and shoulder lift, there was no significant difference in the reduction degree of AHD and AGT in group A with abduction of 0°-30° compared with group B ( P>0.05). The reduction degree of AHD and AGT in group A with abduction of 30°-60°, and the reduction degree of AGT in group A with abduction of 60°-90° were significantly smaller than those in group B ( P<0.05).
Conclusion: In arthroscopic rotator cuff repair, whether the proximal structure of LHBT is cut off or not after LHBT fixation can effectively improve the symptoms of patients and promote the recovery of shoulder joint function. Compared with preserving the proximal structure of LHBT, cutting the proximal structure of LHBT after LHBT fixation has more obvious pain relief within 6 months, and the latter had better stability above the shoulder joint.
目的: 比较关节镜下肩袖修复中肱二头肌长头肌腱(long head of the biceps tendon,LHBT)固定术后近端切断与否,对可修复的肩袖撕裂伴LHBT损伤临床疗效的影响。.
方法: 回顾分析2016年1月—2020年6月符合选择标准的68例LHBT损伤合并冈上肌肌腱撕裂患者临床资料,根据关节镜下肩袖修复中LHBT固定术后近端切断与否分为LHBT固定不切断组(A组,32例)和LHBT固定切断组(B组,36例)。两组患者性别、年龄、手术侧别、术前冈上肌撕裂宽度及Constant-Murley肩关节功能评分量表、美国加州大学洛杉矶分校(UCLA)评分、疼痛视觉模拟评分(VAS)等一般资料比较差异均无统计学意义( P>0.05)。比较两组患者手术时间、屈肘肌力及术后并发症情况;术前及术后3、6、12个月采用Constant-Murley肩关节功能评分量表、UCLA评分、VAS评分评估患肩功能恢复情况;术后即刻及末次随访时通过肩关节Y位X线片测量肩峰间距(acromion-humeral distance,AHD),末次随访时通过肌骨超声测量两组患者患肩外展0°、30°、60° 及90° 时AHD和肩峰-大结节距离(acromion-greater tubercle distance,AGT)。.
结果: 两组手术时间比较差异无统计学意义( t=–0.740, P=0.463)。两组患者均获随访,A、B组随访时间分别为(13.0±0.7)个月和(13.1±0.8)个月,差异无统计学意义( t=0.127, P=0.899)。末次随访时,两组患者屈肘肌力均达Ⅴ级。A组术后6例(18.75%)、B组9例(25.00%)出现并发症(包括患肩疼痛、三角肌萎缩、肩袖再撕裂),均无神经血管损伤、术区感染、关节僵硬、LHBT痉挛痛及Popeye畸形等并发症发生,两组并发症发生率比较差异无统计学意义( χ 2=0.385, P=0.535)。两组患者术后3、6、12个月的Constant-Murley肩关节功能评分量表、UCLA评分及VAS评分均较术前明显改善( P<0.05);术后3、6个月B组上述评分均优于A组( P<0.05),术后12个月两组间比较差异无统计学意义( P>0.05)。肩关节Y位X线片测量示,两组末次随访时AHD均较术后即刻减少,但差值组间比较差异无统计学意义( Z=−1.247, P=0.212);末次随访时A组AHD显著大于B组( t=−2.291, P=0.025)。肌骨超声检测外展抬肩过程中,外展0°-30° A组AHD和AGT减小程度与B组比较差异无统计学意义( P>0.05);外展0°-60° A组AHD和AGT减小程度及外展0°-90° A组AGT减小程度均明显小于B组( P<0.05)。.
结论: 关节镜下肩袖修复中LHBT固定术后近端切断与否均可有效改善患者症状、促进肩关节功能恢复;LHBT固定术后切断LHBT近端结构与保留LHBT近端结构相比,前者6个月内疼痛缓解更明显,后者肩关节上方稳定性更好。.
Keywords: Rotator cuff injury; acromion-humeral distance; long head of the biceps tendon; tenodesis.
Conflict of interest statement
利益冲突 在课题研究和文章撰写过程中不存在利益冲突
Figures
Similar articles
-
[Effectiveness of arthroscopic long head of biceps tendon transposition combined with Swivelock anchor double fixation for massive and irreparable rotator cuff tears].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2022 Dec 15;36(12):1459-1464. doi: 10.7507/1002-1892.202207102. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2022. PMID: 36545852 Free PMC article. Chinese.
-
[Effectiveness of arthroscopic double fixation and enhanced suture of long head of biceps tendon in situ for repairing rotator cuff tear].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2025 Apr 15;39(4):451-456. doi: 10.7507/1002-1892.202501053. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2025. PMID: 40240041 Free PMC article. Chinese.
-
[EFFECTIVENESS OF COMBINED TENODESIS FOR PROXIMAL LESIONS OF BICEPS TENDON WITH MASSIVE ROTATOR CUFF TEAR BY ARTHROSCOPY].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2015 Jun;29(6):667-71. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2015. PMID: 26466465 Chinese.
-
The long head of biceps at the shoulder: a scoping review.BMC Musculoskelet Disord. 2023 Mar 28;24(1):232. doi: 10.1186/s12891-023-06346-5. BMC Musculoskelet Disord. 2023. PMID: 36978047 Free PMC article.
-
Proximal Biceps Tendon and Rotator Cuff Tears.Clin Sports Med. 2016 Jan;35(1):153-61. doi: 10.1016/j.csm.2015.08.010. Epub 2015 Sep 26. Clin Sports Med. 2016. PMID: 26614474 Review.
Cited by
-
[Effectiveness of arthroscopic long head of biceps tendon transposition combined with Swivelock anchor double fixation for massive and irreparable rotator cuff tears].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2022 Dec 15;36(12):1459-1464. doi: 10.7507/1002-1892.202207102. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2022. PMID: 36545852 Free PMC article. Chinese.
References
-
- Nassos JT, Chudik SC Arthroscopic rotator cuff repair with biceps tendon augmentation. Am J Orthop (Belle Mead NJ) 2009;38(6):279–281. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous