

Sex Differences in Mortality of ICU Patients According to Diagnosis-related Sex Balance
- PMID: 35849500
- PMCID: PMC9746862
- DOI: 10.1164/rccm.202203-0539OC
Sex Differences in Mortality of ICU Patients According to Diagnosis-related Sex Balance
Abstract
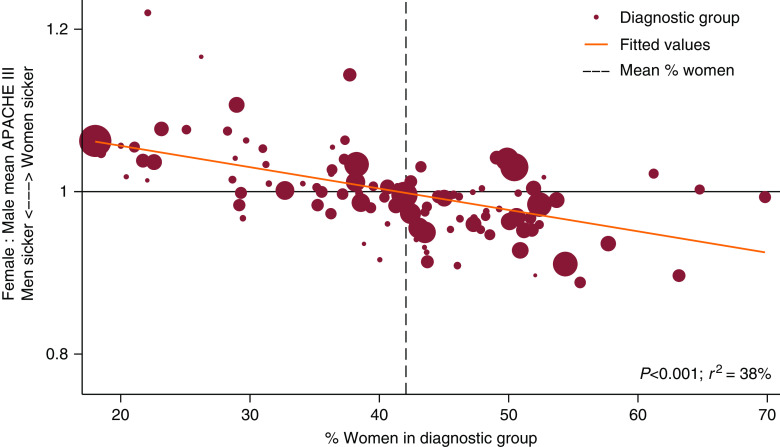
Rationale: Women have worse outcomes than men in several conditions more common in men, including cardiac surgery and burns. Objectives: To describe the relationship between sex balance within each diagnostic group of ICU admissions, defined as the percentage of patients who were women, and hospital mortality of women compared with men with that same diagnosis. Methods: We studied ICU patients in the Australian and New Zealand Intensive Care Society's Adult Patient Database (2011-2020). We performed mixed effects logistic regression for hospital mortality adjusted for sex, illness severity, ICU lead time, admission year, and hospital site. We compared sex balance with the adjusted hospital mortality of women compared with men for each diagnosis using weighted linear regression. Measurements and Main Results: There were 1,450,782 admissions (42.1% women), with no difference in the adjusted hospital mortality of women compared with men overall (odds ratio, 0.99; 99% confidence interval [CI], 0.97 to 1). As the percentage of women within each diagnosis increased, the adjusted mortality of women compared with men with that same diagnosis decreased (regression coefficient, -0.015; 99% CI; -0.020 to -0.011; P < 0.001), and the illness severity of women compared with men at ICU admission decreased (regression coefficient, -0.0026; 99% CI, -0.0035 to -0.0018; P < 0.001). Conclusions: Sex balance in diagnostic groups was inversely associated with both the adjusted mortality and illness severity of women compared with men. In diagnoses with relatively few women, women were more likely than men to die. In diagnoses with fewer men, men were more likely than women to die.
Keywords: illness severity; men; mortality; sex factors; women.
Figures


Comment in
-
Understanding Sex-based Differences in Intensive Care Unit Mortality: Moving Beyond the Biology.Am J Respir Crit Care Med. 2022 Dec 1;206(11):1306-1308. doi: 10.1164/rccm.202207-1443ED. Am J Respir Crit Care Med. 2022. PMID: 35938854 Free PMC article. No abstract available.
References
-
- Moore EC, Pilcher D, Bailey M, Cleland H. Women are more than twice as likely to die from burns as men in Australia and New Zealand: an unexpected finding of the Burns Evaluation And Mortality (BEAM) Study. J Crit Care . 2014;29:594–598. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
