

Effectiveness and safety of acupuncture for postoperative ileus following gastrointestinal surgery: A systematic review and meta-analysis
- PMID: 35849611
- PMCID: PMC9292096
- DOI: 10.1371/journal.pone.0271580
Effectiveness and safety of acupuncture for postoperative ileus following gastrointestinal surgery: A systematic review and meta-analysis
Abstract
Background: Postoperative ileus (POI) is an important complication of gastrointestinal (GI) surgery. Acupuncture has been increasingly used in treating POI. This study aimed to assess the effectiveness and safety of acupuncture for POI following GI surgery.
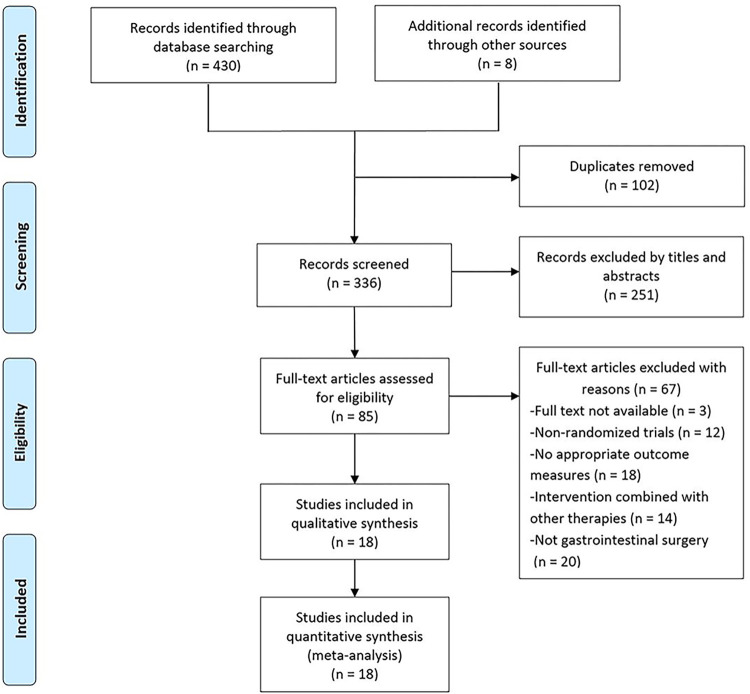
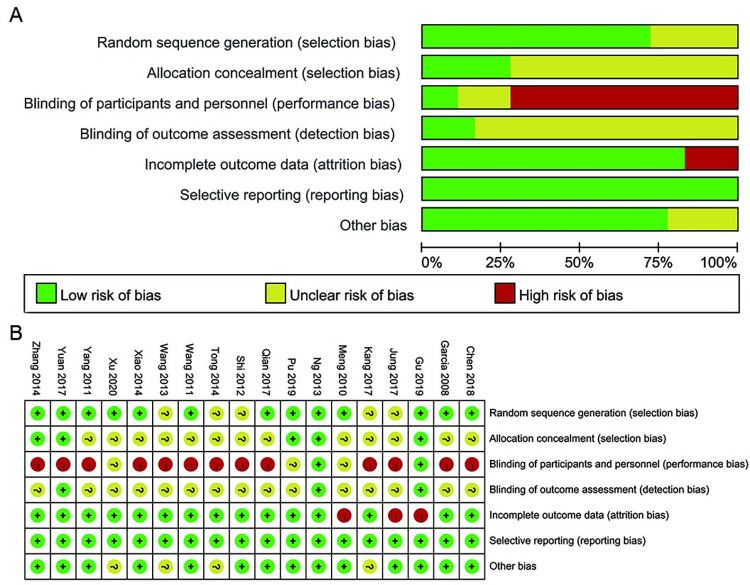
Methods: Seven databases (PubMed, Embase, the Cochrane Library, China National Knowledge Infrastructure, Wan fang Data, VIP Database for Chinese Technical Periodicals, and Chinese Biomedical Literature Database) and related resources were searched from inception to May 30, 2021. Randomized controlled trials (RCTs) reporting the acupuncture for POI in GI were included. The quality of RCTs was assessed by the Cochrane Collaboration Risk of Bias tool, and the certainty of the evidence was evaluated by the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) approach. A meta-analysis was performed by using RevMan 5.4 software.
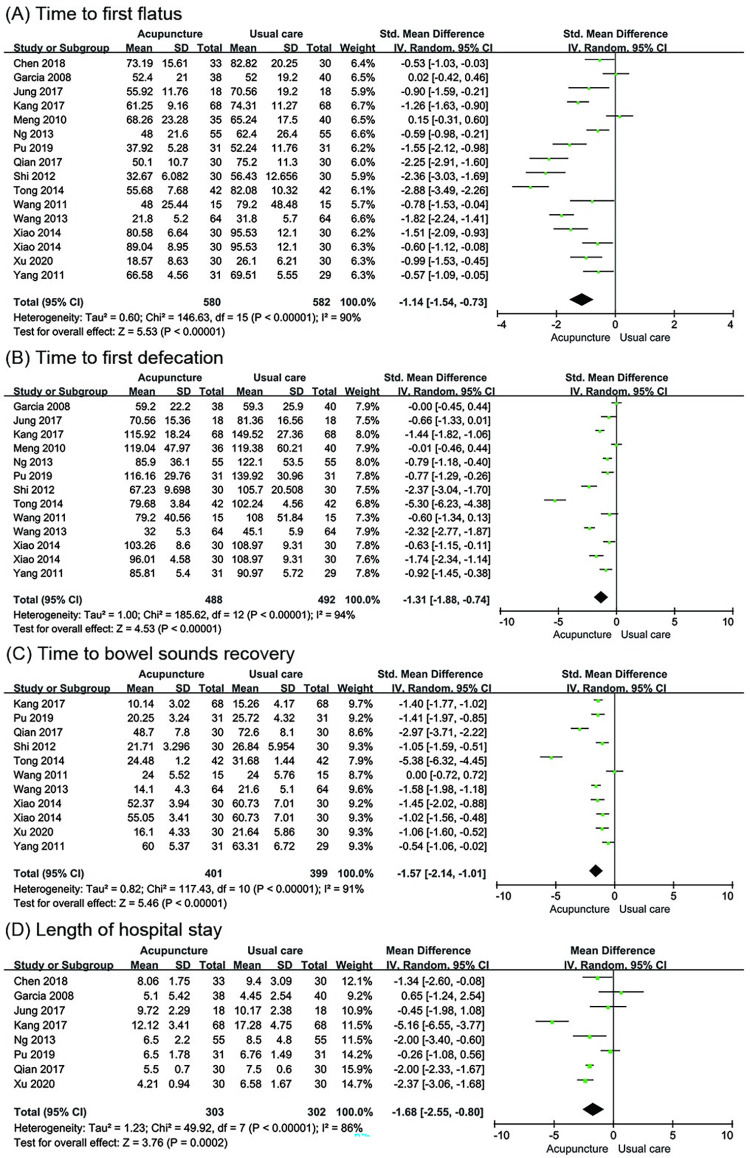
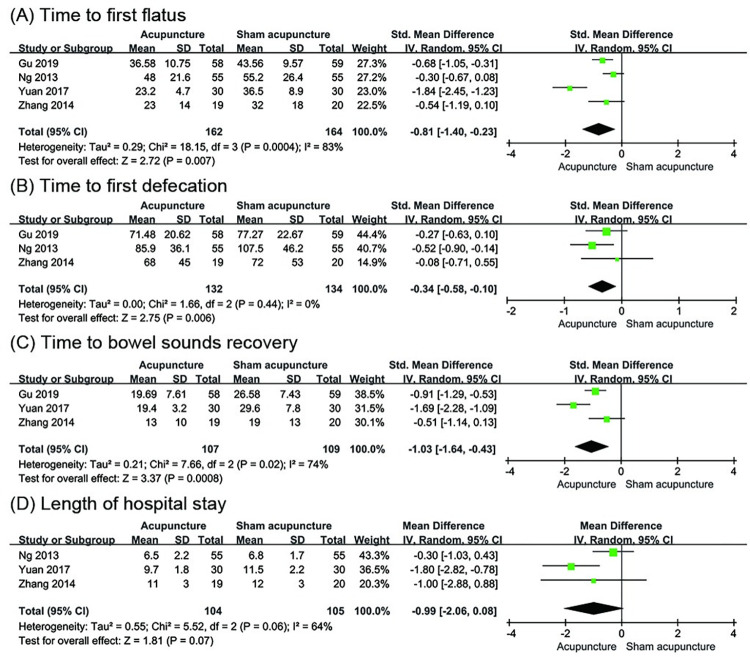
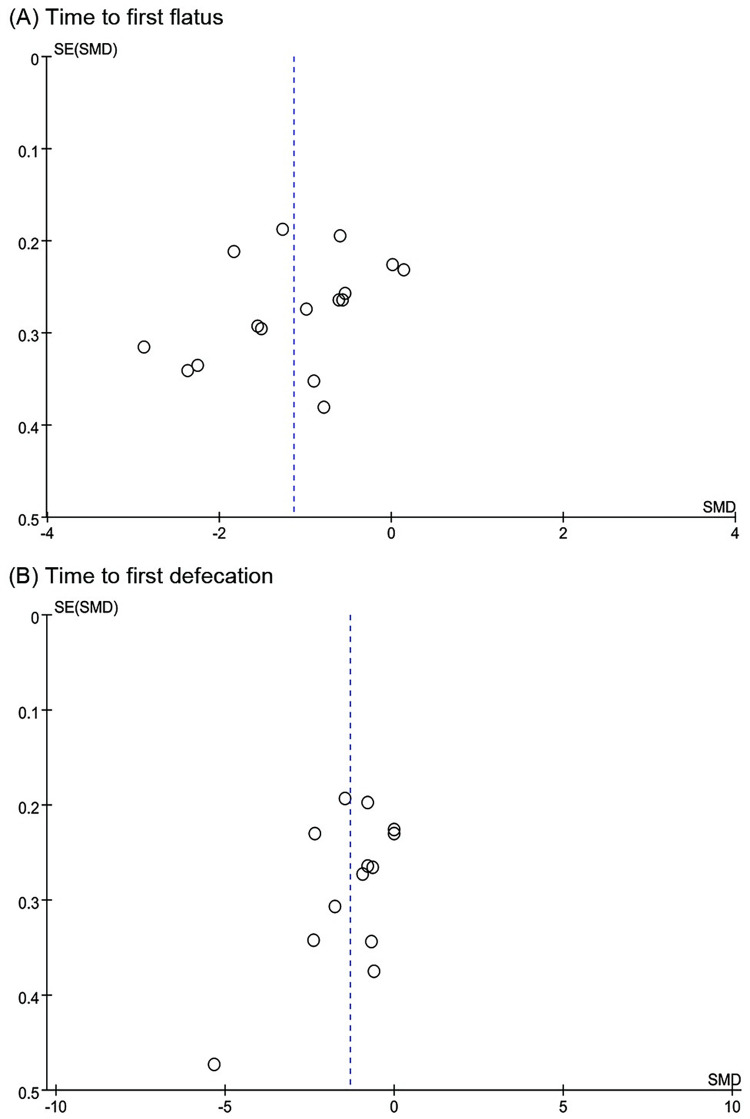
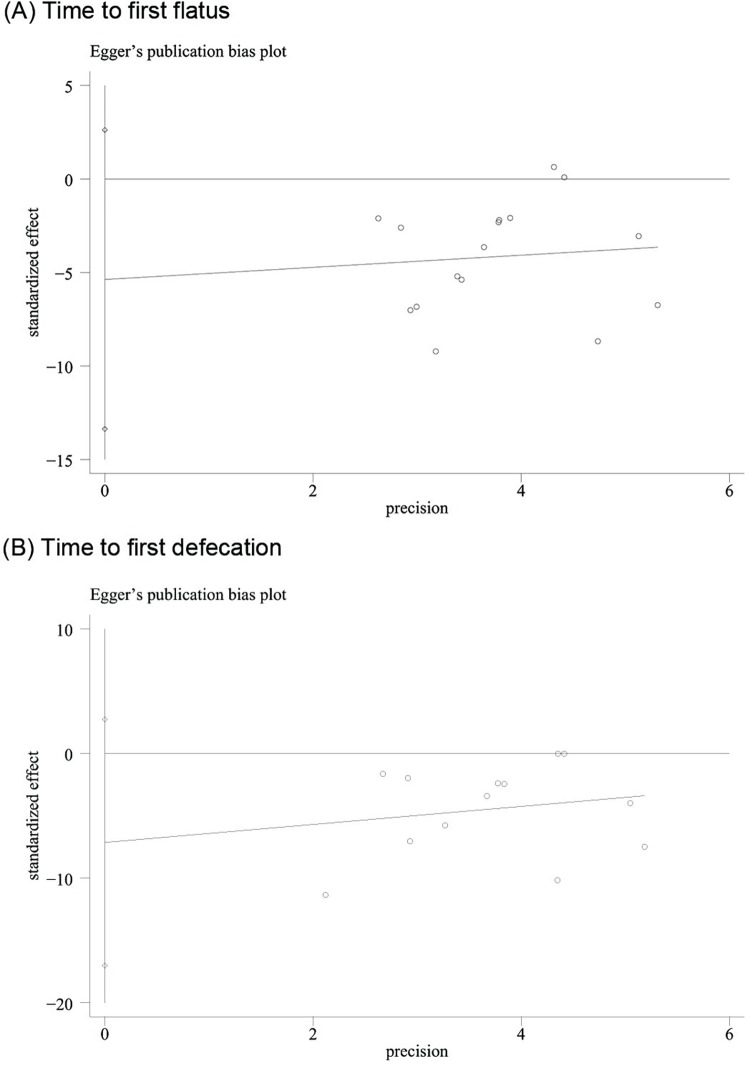
Results: Eighteen RCTs involving 1413 participants were included. The meta-analysis showed that acupuncture could reduce the time to first flatus (TFF) (standardized mean difference [SMD] = -1.14, 95% confidence interval [CI]: -1.54 to -0.73, P < 0.00001), time to first defecation (TFD) (SMD = -1.31, 95% CI: -1.88 to -0.74, P < 0.00001), time to bowel sounds recovery (TBSR) (SMD = -1.57, 95% CI: -2.14 to -1.01, P < 0.00001), and length of hospital stay (LOS) (mean difference [MD] = -1.68, 95% CI: -2.55 to -0.80, P = 0.0002) compared with usual care. A subgroup analysis found that acupuncture at distal acupoints once daily after surgery had superior effects on reducing TFF and TFD. A sensitivity analysis supported the validity of the finding. Acupuncture also manifested an effect of reducing TFF, TFD and TBSR compared with sham acupuncture but the result was not stable. Relatively few trials have reported whether adverse events have occurred.
Conclusions: Acupuncture showed a certain effect in reducing POI following GI surgery with very low-to-moderate quality of evidence. The overall safety of acupuncture should be further validated. More high-quality, large-scale, and multicenter original trials are needed in the future.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Acupuncture for postoperative gastrointestinal dysfunction in cancer: a systematic review and meta-analysis.Front Oncol. 2023 Jun 9;13:1184228. doi: 10.3389/fonc.2023.1184228. eCollection 2023. Front Oncol. 2023. PMID: 37361600 Free PMC article.
-
Efficacy and safety of acupuncture in postoperative ileus after gynecological surgery: A protocol for system review and meta-analysis of randomized controlled trials.Medicine (Baltimore). 2021 Feb 5;100(5):e24342. doi: 10.1097/MD.0000000000024342. Medicine (Baltimore). 2021. PMID: 33592880 Free PMC article.
-
Acupuncture for enhancing early recovery of bowel function in cancer: Protocol for a systematic review.Medicine (Baltimore). 2017 Apr;96(17):e6644. doi: 10.1097/MD.0000000000006644. Medicine (Baltimore). 2017. PMID: 28445263 Free PMC article.
-
Does invasive acupuncture improve postoperative ileus after colorectal cancer surgery? A systematic review and meta-analysis.Front Med (Lausanne). 2023 Aug 25;10:1201769. doi: 10.3389/fmed.2023.1201769. eCollection 2023. Front Med (Lausanne). 2023. PMID: 37692781 Free PMC article. Review.
-
Electroacupuncture or transcutaneous electroacupuncture for postoperative ileus after abdominal surgery: A systematic review and meta-analysis.Int J Surg. 2019 Oct;70:93-101. doi: 10.1016/j.ijsu.2019.08.034. Epub 2019 Sep 5. Int J Surg. 2019. PMID: 31494334
Cited by
-
Efficacy of electroacupuncture in improving postoperative ileus in patients receiving colorectal surgery: a systematic review and meta-analysis.Int J Surg. 2024 Feb 1;110(2):1113-1125. doi: 10.1097/JS9.0000000000000848. Int J Surg. 2024. PMID: 37916930 Free PMC article.
-
The State of 21st Century Acupuncture in the United States.J Pain Res. 2024 Oct 10;17:3329-3354. doi: 10.2147/JPR.S469491. eCollection 2024. J Pain Res. 2024. PMID: 39403098 Free PMC article.
-
Acupuncture for postoperative ileus: Advancement and underlying mechanisms.World J Gastrointest Surg. 2025 Feb 27;17(2):99160. doi: 10.4240/wjgs.v17.i2.99160. World J Gastrointest Surg. 2025. PMID: 40061996 Free PMC article.
-
Clinical observation of gastrointestinal function recovery in patients after hepatobiliary surgery.World J Gastrointest Surg. 2024 Jan 27;16(1):76-84. doi: 10.4240/wjgs.v16.i1.76. World J Gastrointest Surg. 2024. PMID: 38328324 Free PMC article.
-
The effect of acupuncture on recovery after colorectal cancer resection: A systematic review meta-analysis of randomized controlled trials.Medicine (Baltimore). 2023 Sep 1;102(35):e34678. doi: 10.1097/MD.0000000000034678. Medicine (Baltimore). 2023. PMID: 37657054 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
