

Burden of diabetes and hyperglycaemia in adults in the Americas, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019
- PMID: 35850129
- PMCID: PMC9399220
- DOI: 10.1016/S2213-8587(22)00186-3
Burden of diabetes and hyperglycaemia in adults in the Americas, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019
Abstract
Background: High prevalence of diabetes has been reported in the Americas, but no comprehensive analysis of diabetes burden and related factors for the region is available. We aimed to describe the burden of type 1 and type 2 diabetes and that of hyperglycaemia in the Americas from 1990 to 2019.
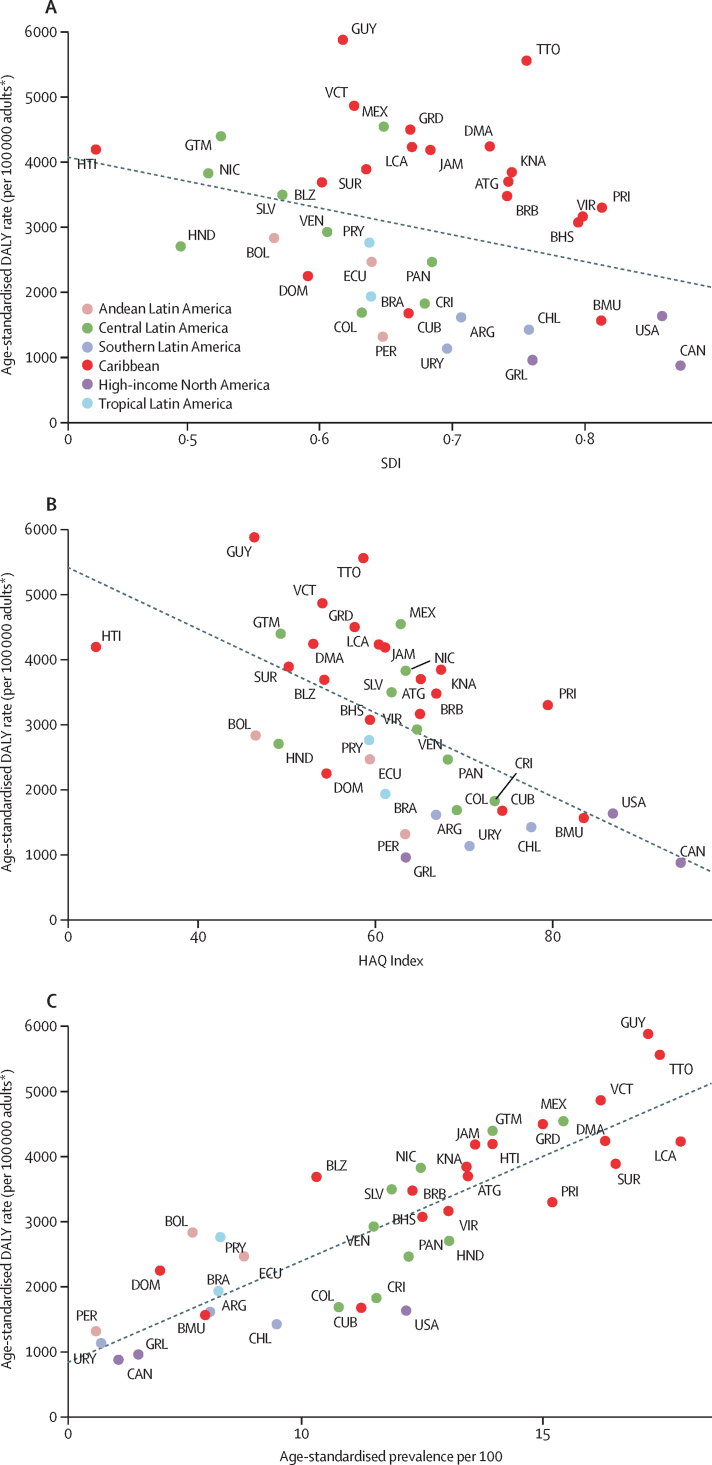
Methods: We used estimates from GBD 2019 to evaluate the burden of diabetes in adults aged 20 years or older and high fasting plasma glucose in adults aged 25 years or older in the 39 countries and territories of the six regions in the Americas from 1990 to 2019. The main source to estimate the mortality attributable to diabetes and to chronic kidney disease due to diabetes was vital registration. Mortality due to overall diabetes (ie, diabetes and diabetes due to chronic kidney disease) was estimated using the Cause of Death Ensemble model. Years of life lost (YLLs) were calculated as the number of deaths multiplied by standard life expectancy at the age that the death occurred, years lived with disability (YLDs) were estimated based on the prevalence and severity of complications of diabetes. Disability-adjusted life-years (DALYs) were estimated as a sum of YLDs and YLLs. We assessed the association of diabetes burden with the level of development of a country (according to the Socio-demographic Index), health-care access and quality (estimated with the Healthcare Access and Quality Index), and diabetes prevalence. We also calculated the population attributable fraction (PAF) of diabetes burden due to each of its risk factors. We report the 95% uncertainty intervals for all estimates.
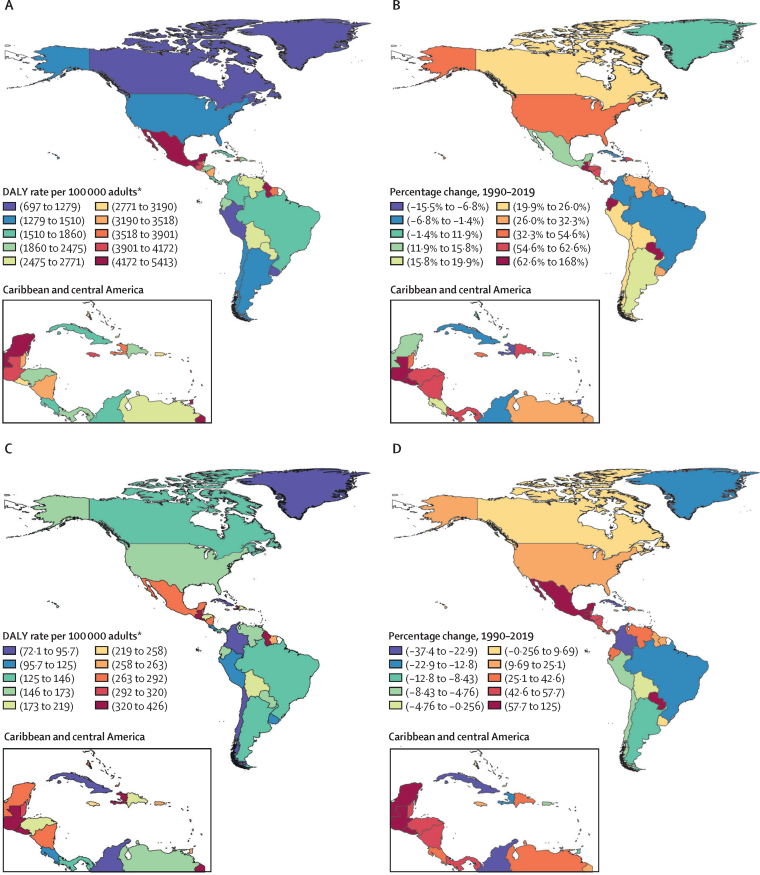
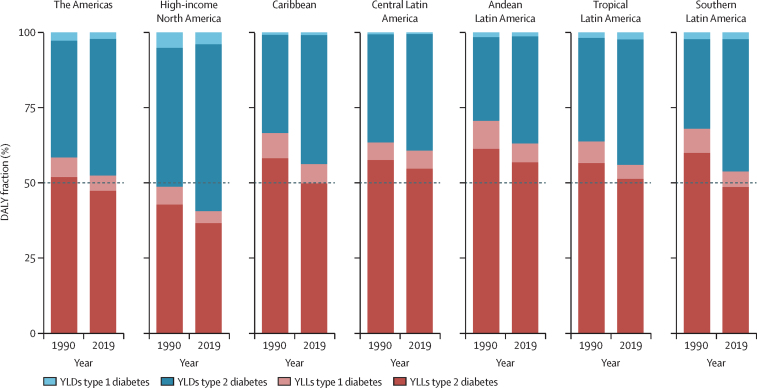
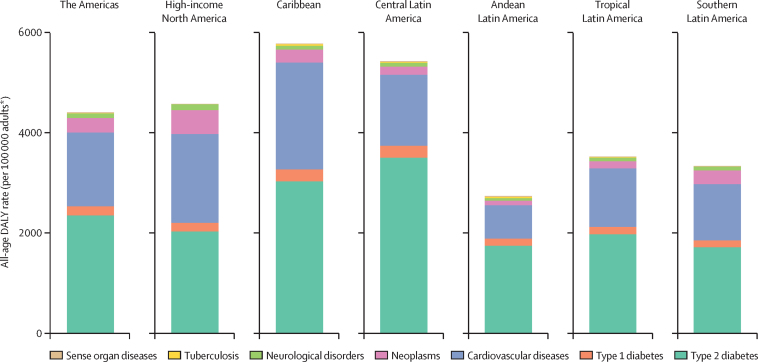
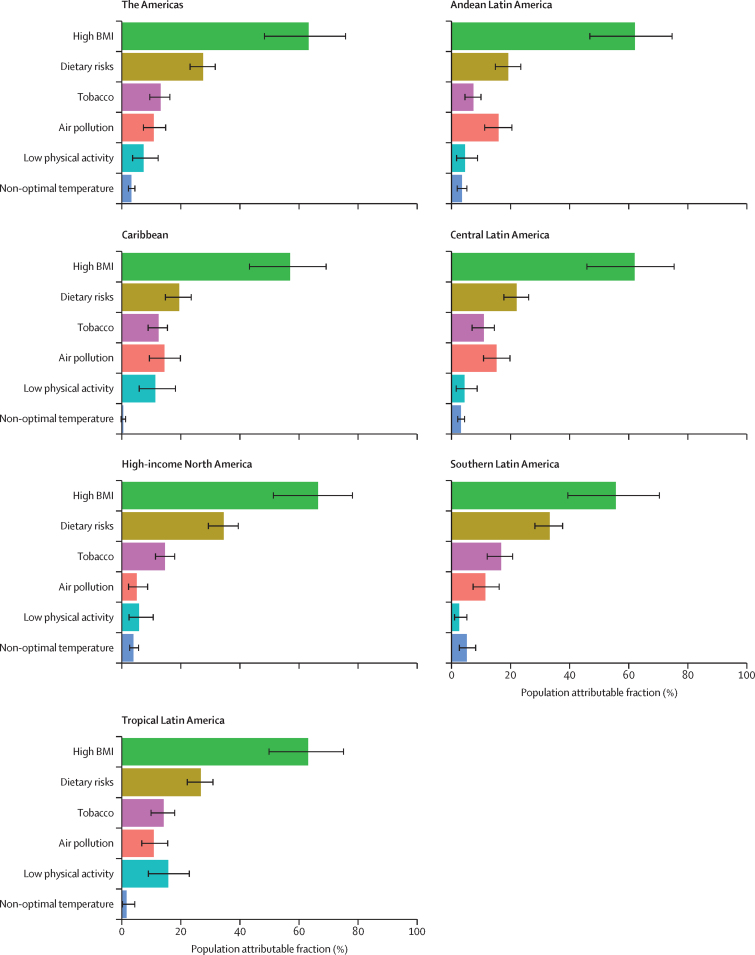
Findings: In 2019, an estimated total of 409 000 (95% uncertainty interval 373 000-443 000) adults aged 20 years or older in the Americas died from diabetes, which represented 5·9% of all deaths. Diabetes was responsible for 2266 (1930-2649) crude DALYs per 100 000 adults in the Americas, and high fasting plasma glucose for 4401 DALYs (3685-5265) per 100 000 adults, with large variation across regions. DALYs were mostly due to type 2 diabetes and distribution was heterogeneous, being highest in central Latin America and the Caribbean and lowest in high-income North America and southern Latin America. Between 1990 and 2019, age-standardised DALYs due to type 2 diabetes increased 27·4% (22·0-32·5). This increase was particularly high in Andean Latin America and high-income North America. Burden for both type 1 and type 2 diabetes across countries increased with higher diabetes prevalence and decreased with greater Socio-demographic and Healthcare Access and Quality Indices. Main risk factors for the burden were high BMI, with a PAF of 63·2% and dietary risks, with a PAF of 27·5%. The fraction of burden due to disability has increased since 1990 and now represents nearly half of the overall burden in 2019.
Interpretation: The burden of diabetes in the Americas is large, increasing, heterogeneous, and expanding. To confront the rising burden, population-based interventions aimed to reduce type 2 diabetes risk and strengthening health systems to provide effective and cost-efficient care for those affected are mandatory.
Funding: Bill & Melinda Gates Foundation.
Copyright © 2022 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests T Bärnighausen reports support for the present manuscript from Alexander von Humboldt Foundation, Wellcome Trust, German Research Foundation, and US National Institutes of Health (National Institute of Allergy and Infectious Diseases, National Institute on Aging, and Fogarty International Center), paid to his institution. I Filip and A Radfar report support from Avicenna Medical and Clinical Research Institute, outside the submitted work. J A Singh reports consulting fees from Crealta/Horizon, Medisys, Fidia, PK Med, Two labs, Adept Field Solutions, Clinical Care Options, Clearview Healthcare Partners, Putnam Associates, Focus Forward, Navigant Consulting, Spherix, MedIQ, Jupiter Life Science, UBM, Trio Health, Medscape, WebMD, and Practice Point Communications, the National Institutes of Health, and the American College of Rheumatology; payment or honoraria for lectures, presentations, speakers' bureaus, manuscript writing or educational events from Simply Speaking; support for attending meetings or travel from the steering committee of OMERACT; participation on a Data Safety Monitoring Board or Advisory Board with the US Food and Drug Administration Arthritis Advisory Committee; leadership or fiduciary role in board, society, committee or advocacy group, paid or unpaid, with OMERACT as a steering committee member, with the Veterans Affairs Rheumatology Field Advisory Committee as Chair (unpaid), and with the UAB Cochrane Musculoskeletal Group Satellite Center on Network Meta-analysis and editor and director (unpaid); stock or stock options in TPT Global Tech, Vaxart Pharmaceuticals, Atyu Biopharma, Adaptimmune Therapeutics, GeoVax Labs, Pieris Pharmaceuticals, Enzolytics, Seres Therapeutics, Tonix Pharmaceuticals and Charlotte's Web Holdings, and previously owned stock options in Amarin, Viking and Moderna Pharmaceuticals; all outside the submitted work.
Figures
Comment in
-
The burden of diabetes in the Americas.Lancet Diabetes Endocrinol. 2022 Sep;10(9):613-614. doi: 10.1016/S2213-8587(22)00196-6. Epub 2022 Jul 15. Lancet Diabetes Endocrinol. 2022. PMID: 35850130 No abstract available.
References
-
- WHO General meeting of the WHO global coordination mechanism on the prevention and control of noncommunicable diseases: meeting report. International Conference Centre, Geneva, Switzerland, 5-6 November 2018. 2019. https://apps.who.int/iris/handle/10665/310961
-
- International Diabetes Federation IDF Diabetes Atlas, 9th edn. 2019. https://www.diabetesatlas.org/en/
