

Patterns of Use, Outcomes, and Resource Utilization among Recipients of Commercial Axicabtagene Ciloleucel and Tisagenlecleucel for Relapsed/Refractory Aggressive B Cell Lymphomas
- PMID: 35850429
- PMCID: PMC9547952
- DOI: 10.1016/j.jtct.2022.07.011
Patterns of Use, Outcomes, and Resource Utilization among Recipients of Commercial Axicabtagene Ciloleucel and Tisagenlecleucel for Relapsed/Refractory Aggressive B Cell Lymphomas
Abstract
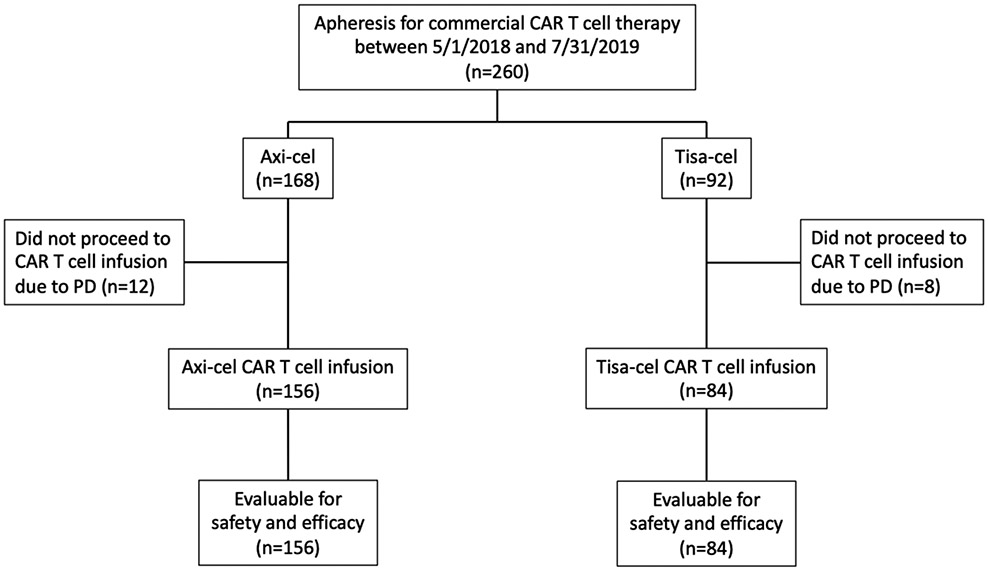
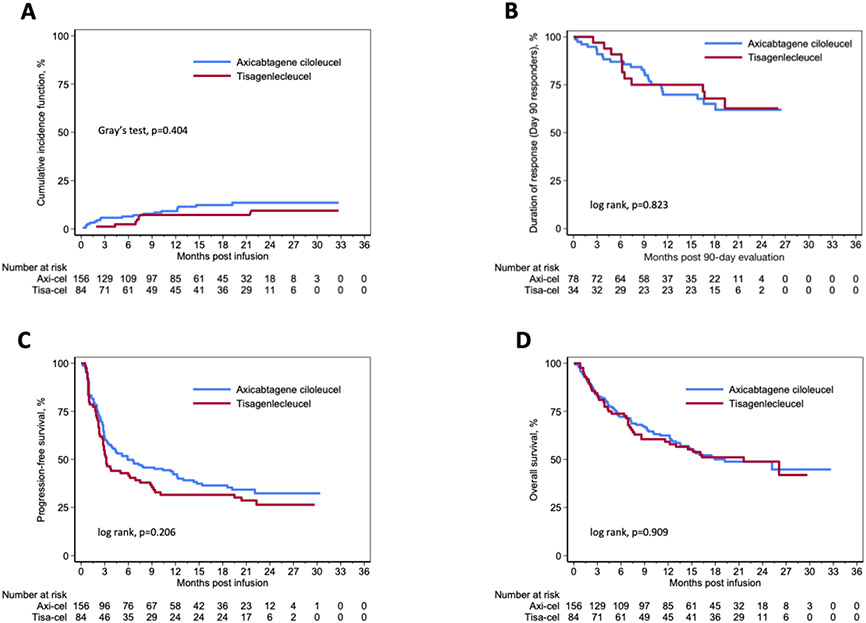
Axicabtagene ciloleucel (axi-cel) and tisagenlecleucel (tisa-cel) are CD19-directed chimeric antigen receptor (CAR) T cell therapies approved for the treatment of relapsed/refractory aggressive B cell lymphomas. We present a multicenter retrospective study among centers that prescribe either commercial product to evaluate usage patterns, safety and efficacy outcomes, and resource utilization. Data collection included all patients from 8 US centers who underwent apheresis between May 1, 2018, and July 31, 2019. Patient selection, toxicity management, and disease assessment followed institutional practices. Cytokine release syndrome (CRS) and immune effector cell-associated neurotoxicity syndrome (ICANS) were graded according to American Society for Transplantation and Cellular Therapy consensus criteria, and tumor responses were assessed according to the Lugano 2014 classification scheme. A total of 260 patients underwent apheresis, including 168 (65%) for axi-cel and 92 (35%) for tisa-cel. Among the infused patients, the median age was 59 years for axi-cel recipients and 67 years for tisa-cel recipients (P < .001). The median time from apheresis to infusion was 28 days for axi-cel recipients and 45 days for tisa-cel recipients (P < .001). Sixty-one percent of the axi-cel recipients and 43% of the tisa-cel recipients would have been ineligible for the ZUMA-1 and JULIET trials, respectively. Grade ≥3 CRS occurred in 9% of axi-cel recipients and in 1% of tisa-cel recipients (P = .017), and grade ≥3 ICANS was seen in 38% of axi-cel recipients and 1% of tisa-cel recipients (P < .001). Inpatient cell therapy infusion was common (92% in axi-cel recipients, 37% in tisa-cel recipients). The day 90 overall response rate was 52% in the axi-cel group and 41% in the tisa-cel group (P = .113), with complete response in 44% and 35%, respectively (P = .319). Twelve-month progression-free survival (42% versus 32%; P = .206) and overall survival (62% versus 59%; P = .909) rates were comparable in the axi-cel and tisa-cel groups. Baseline characteristics differed between the 2 groups, although response rates and survival outcomes were comparable, albeit lower than those in the pivotal trials. Safety and resource utilization appear to be key differentiators between axi-cel and tisa-cel.
Keywords: Aggressive large B cell lymphoma; CAR T cell therapy outcomes; CAR T cell toxicity; Chimeric antigen receptor T cell therapy; Resource utilization.
Copyright © 2022 The American Society for Transplantation and Cellular Therapy. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
CONFLICTS OF INTEREST DISCLOSURES:
Figures
Comment in
-
Choosing a CAR for Relapsed/Refractory Large B-cell Lymphoma.Transplant Cell Ther. 2022 Oct;28(10):621-622. doi: 10.1016/j.jtct.2022.09.006. Transplant Cell Ther. 2022. PMID: 36202524 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
