

Artificial intelligence fully automated myocardial strain quantification for risk stratification following acute myocardial infarction
- PMID: 35851282
- PMCID: PMC9293901
- DOI: 10.1038/s41598-022-16228-w
Artificial intelligence fully automated myocardial strain quantification for risk stratification following acute myocardial infarction
Abstract
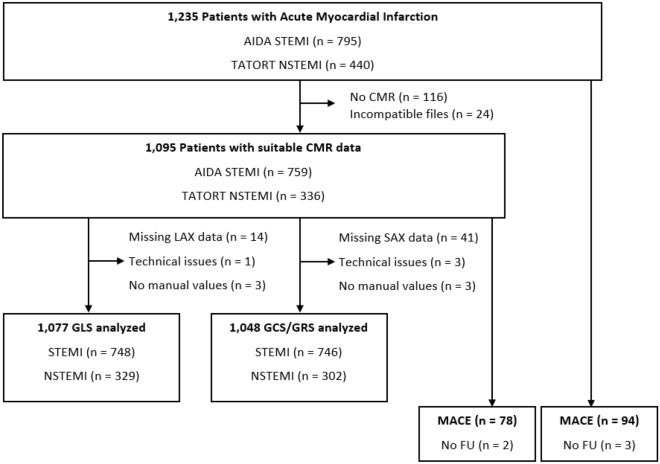
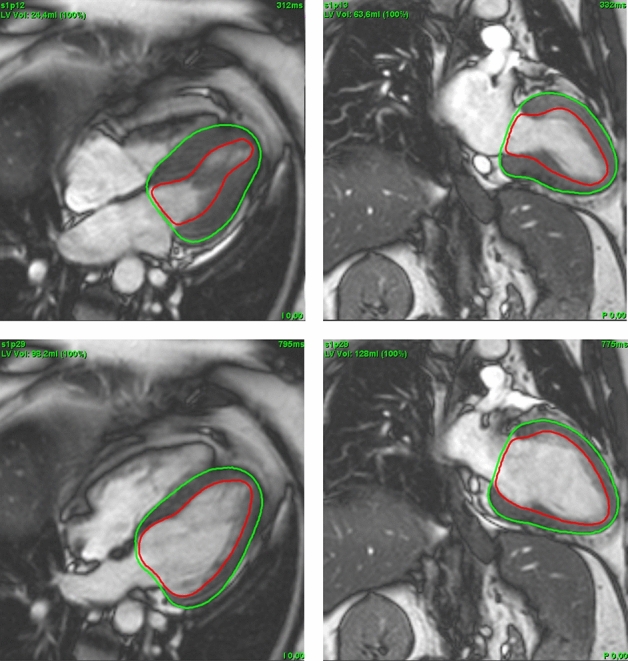
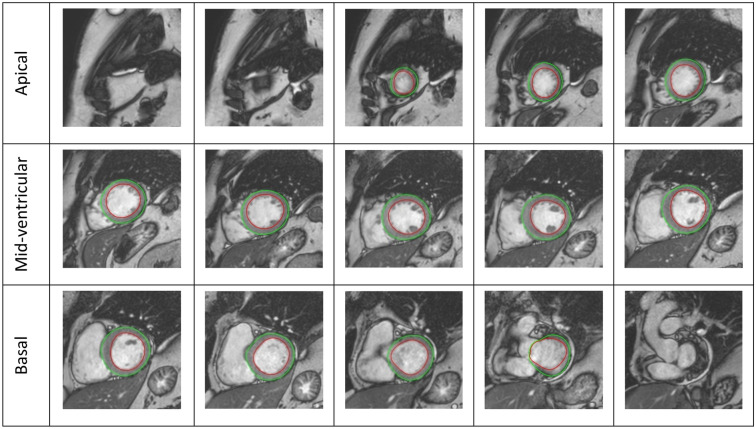
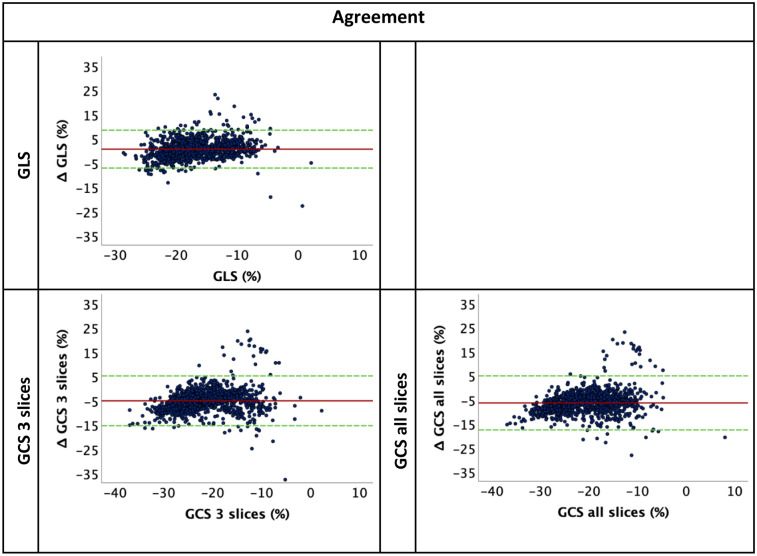
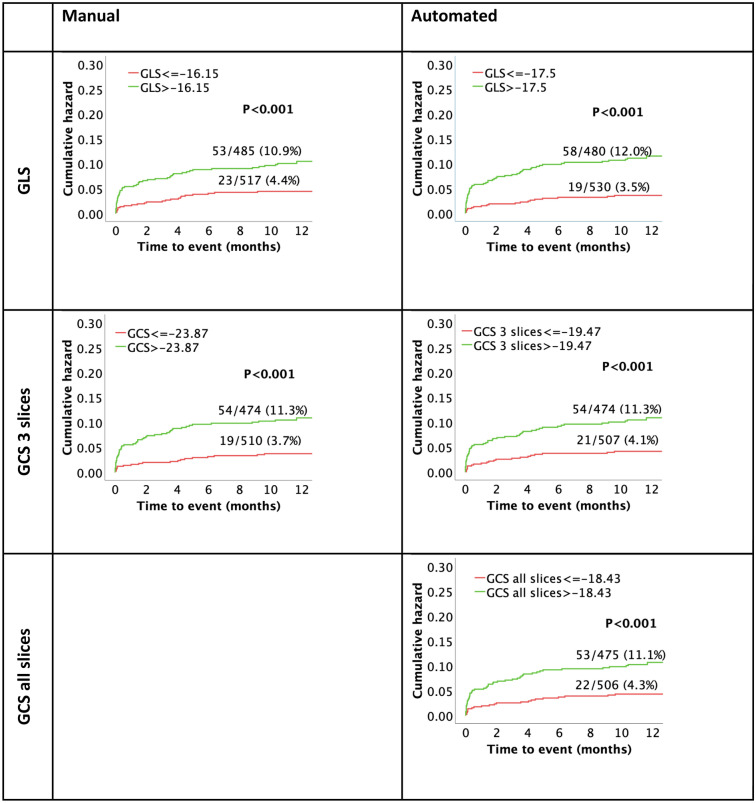
Feasibility of automated volume-derived cardiac functional evaluation has successfully been demonstrated using cardiovascular magnetic resonance (CMR) imaging. Notwithstanding, strain assessment has proven incremental value for cardiovascular risk stratification. Since introduction of deformation imaging to clinical practice has been complicated by time-consuming post-processing, we sought to investigate automation respectively. CMR data (n = 1095 patients) from two prospectively recruited acute myocardial infarction (AMI) populations with ST-elevation (STEMI) (AIDA STEMI n = 759) and non-STEMI (TATORT-NSTEMI n = 336) were analysed fully automated and manually on conventional cine sequences. LV function assessment included global longitudinal, circumferential, and radial strains (GLS/GCS/GRS). Agreements were assessed between automated and manual strain assessments. The former were assessed for major adverse cardiac event (MACE) prediction within 12 months following AMI. Manually and automated derived GLS showed the best and excellent agreement with an intraclass correlation coefficient (ICC) of 0.81. Agreement was good for GCS and poor for GRS. Amongst automated analyses, GLS (HR 1.12, 95% CI 1.08-1.16, p < 0.001) and GCS (HR 1.07, 95% CI 1.05-1.10, p < 0.001) best predicted MACE with similar diagnostic accuracy compared to manual analyses; area under the curve (AUC) for GLS (auto 0.691 vs. manual 0.693, p = 0.801) and GCS (auto 0.668 vs. manual 0.686, p = 0.425). Amongst automated functional analyses, GLS was the only independent predictor of MACE in multivariate analyses (HR 1.10, 95% CI 1.04-1.15, p < 0.001). Considering high agreement of automated GLS and equally high accuracy for risk prediction compared to the reference standard of manual analyses, automation may improve efficiency and aid in clinical routine implementation.Trial registration: ClinicalTrials.gov, NCT00712101 and NCT01612312.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Roffi M, et al. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC) Eur. Heart J. 2016;37(3):267–315. doi: 10.1093/eurheartj/ehv320. - DOI - PubMed
-
- Epstein AE, et al. ACC/AHA/HRS 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the ACC/AHA/NASPE 2002 Guideline Update for Implantation of Cardiac Pacemakers and Antiarrhythmia Devices): Developed in collaboration with the American Association for Thoracic Surgery and Society of Thoracic Surgeons. Circulation. 2008;117(21):e350–e408. doi: 10.1161/CIRCUALTIONAHA.108.189742. - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
