

Acute skeletal muscle loss in SARS-CoV-2 infection contributes to poor clinical outcomes in COVID-19 patients
- PMID: 35851995
- PMCID: PMC9350025
- DOI: 10.1002/jcsm.13052
Acute skeletal muscle loss in SARS-CoV-2 infection contributes to poor clinical outcomes in COVID-19 patients
Abstract
Background: Chronic disease causes skeletal muscle loss that contributes to morbidity and mortality. There are limited data on the impact of dynamic muscle loss on clinical outcomes in COVID-19. We hypothesized that acute COVID-19-related muscle loss (acute sarcopenia) is associated with adverse outcomes.
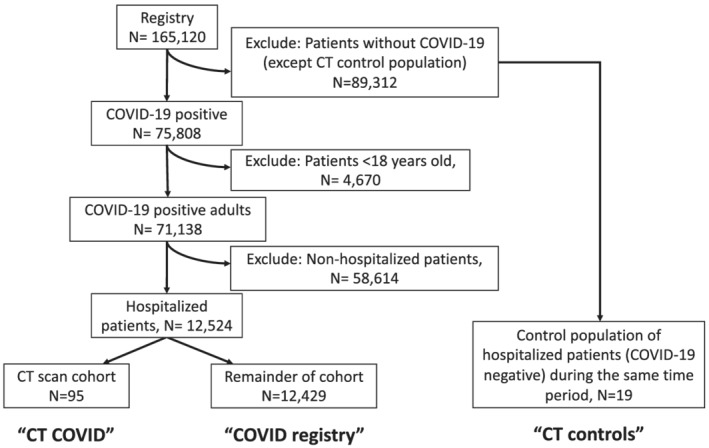
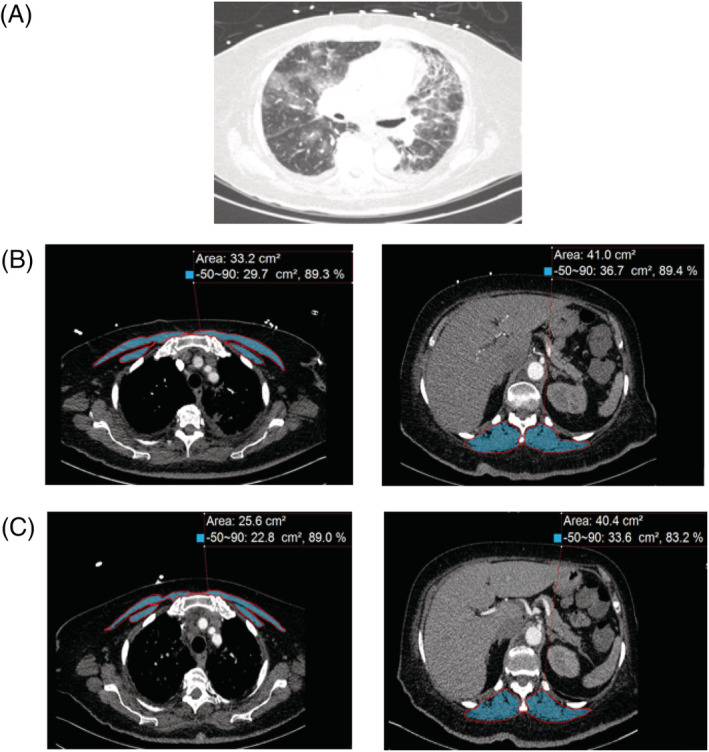
Methods: A retrospective analysis of a prospective clinical registry of COVID-19 patients was performed in consecutive hospitalized patients with acute COVID-19 (n = 95) and compared with non-COVID-19 controls (n = 19) with two temporally unique CT scans. Pectoralis muscle (PM), erector spinae muscle (ESM) and 30 day standardized per cent change in cross sectional muscle area were quantified. Primary outcomes included mortality and need for intensive care unit (ICU) admission. Multivariate linear and logistic regression were performed. Cox proportional hazard ratios were generated for ICU admission or mortality for the per cent muscle loss standardized to 30 days.
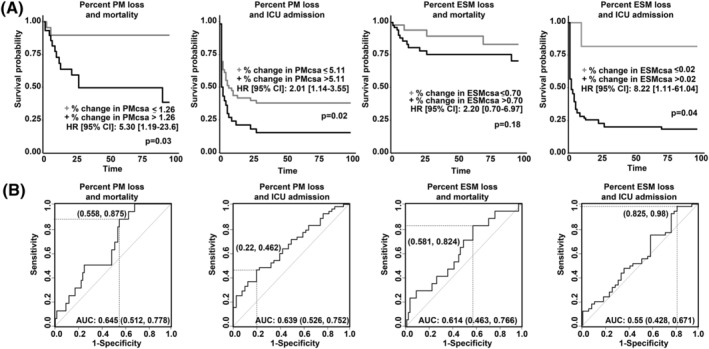
Results: The COVID-19 CT scan cohort (n = 95) had an average age of 63.3 ± 14.3 years, comorbidities including COPD (28.4%) and diabetes mellitus (42.1%), and was predominantly Caucasian (64.9%). The proportion of those admitted to the ICU was 54.7%, with 10.5% requiring tracheostomy and overall mortality 16.8%. Median duration between CT scans was 32 days (IQR: 16-63 days). Significant reductions in median per cent loss was noted for PM (-2.64% loss [IQR: -0.28, -5.47] in COVID-19 vs. -0.06 loss [IQR: -0.01, -0.28] in non-COVID-19 CT controls, P < 0.001) and ESM (-1.86% loss [IQR: -0.28, -5.47] in COVID-19 vs. -0.06 loss [IQR: -0.02, -0.11]) in non-COVID-19 CT controls, P < 0.001). Multivariate linear regression analysis of per cent loss in PM was significantly associated with mortality (-10.8% loss [95% CI: -21.5 to -0.19]) and ICU admission (-11.1% loss [95% CI: -19.4 to -2.67]), and not significant for ESM. Cox proportional hazard ratios demonstrated greater association with ICU admission (adj HR 2.01 [95% CI: 1.14-3.55]) and mortality (adj HR 5.30 [95% CI: 1.19-23.6]) for those with significant per cent loss in PM, and greater association with ICU admission (adj HR 8.22 [95% CI: 1.11-61.04]) but not mortality (adj HR 2.20 [95% CI: 0.70-6.97]) for those with significant per cent loss in ESM.
Conclusions: In a well-characterized cohort of 95 hospitalized patients with acute COVID-19 and two temporally distinct CT scans, acute sarcopenia, determined by standardized reductions in PM and ESM, was associated with worse clinical outcomes. These data lay the foundation for evaluating dynamic muscle loss as a predictor of clinical outcomes and targeting acute sarcopenia to improve clinical outcomes for COVID-19.
Keywords: Acute sarcopenia; COVID-19; Erector spinae muscle area; Standardized reduction; pectoralis muscle area.
© 2022 The Authors. Journal of Cachexia, Sarcopenia and Muscle published by John Wiley & Sons Ltd on behalf of Society on Sarcopenia, Cachexia and Wasting Disorders.
Conflict of interest statement
The authors have no other conflicts of interest other than the grants listed above. The funders did not have any role in the design, analysis or interpretation of the data.
Figures
References
-
- Puthucheary ZA, Rawal J, McPhail M, Connolly B, Ratnayake G, Chan P, et al. Acute skeletal muscle wasting in critical illness. JAMA 2013;310:1591–1600. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
