

Adding Umbralisib and Ublituximab (U2) to Ibrutinib in Patients with CLL: A Phase II Study of an MRD-Driven Approach
- PMID: 35852793
- PMCID: PMC9481719
- DOI: 10.1158/1078-0432.CCR-22-0964
Adding Umbralisib and Ublituximab (U2) to Ibrutinib in Patients with CLL: A Phase II Study of an MRD-Driven Approach
Abstract
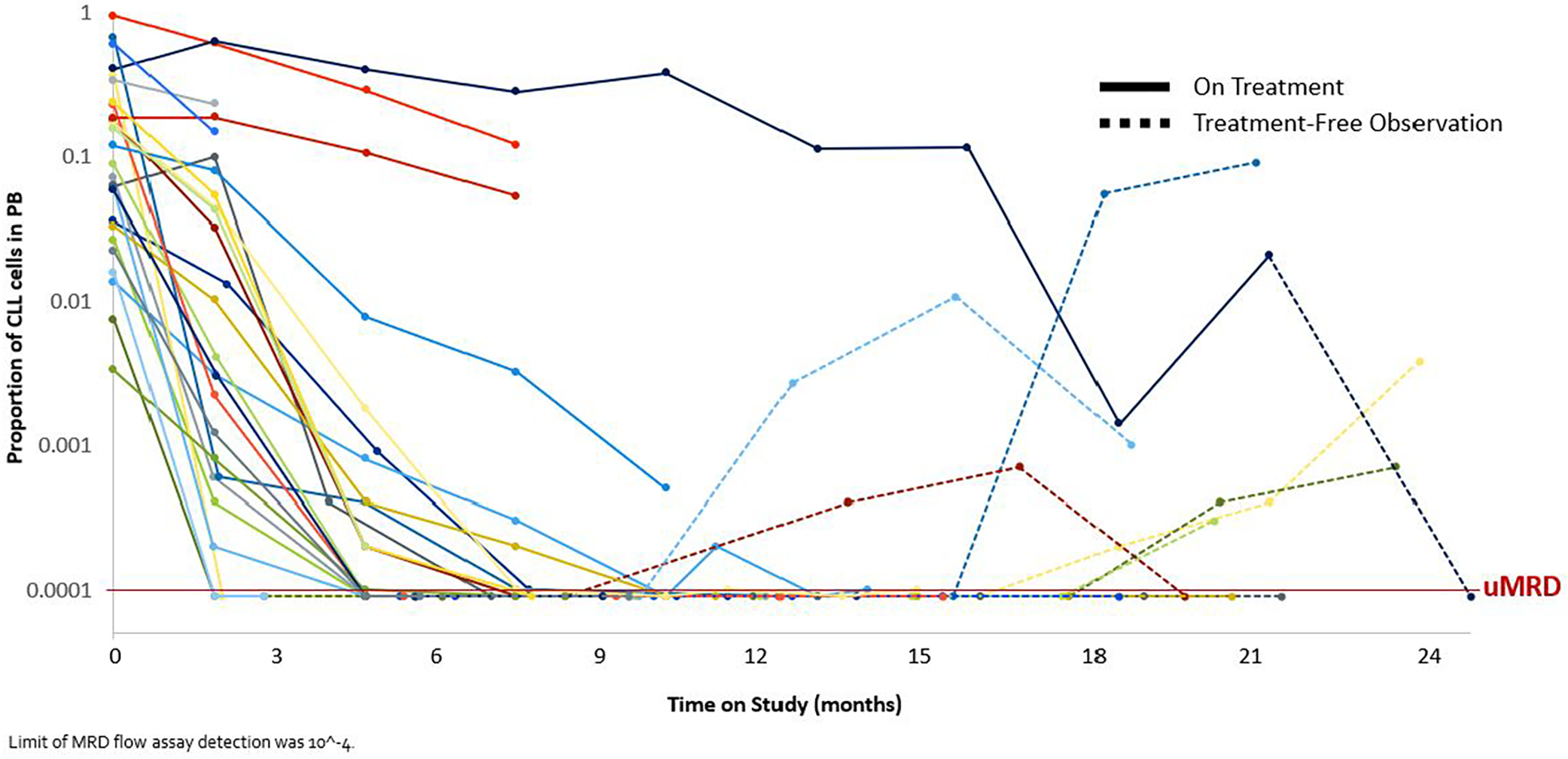
Purpose: Ibrutinib has transformed the management of chronic lymphocytic leukemia (CLL), though its use is limited by toxicity and resistance. In this study, we utilized an "add on" approach for patients who had been treated with ibrutinib in the front-line or relapsed/refractory settings with detectable MRD. Umbralisib and ublituximab (U2) were added on to ibrutinib, patients were treated until achieving undetectable-MRD (U-MRD), and then they entered a period of treatment-free observation (TFO).
Patients and methods: Patients were eligible if they received ibrutinib in any line of therapy for at least 6 months and had detectable MRD (flow cytometry, <1 cell in 10-4 cutoff for U-MRD). U2 was added to ibrutinib, and patients were monitored serially for MRD. Once U-MRD was achieved or a total of 24 cycles were administered, patients entered a period of TFO. The primary study objective was rate of U-MRD. Secondary endpoints included safety and durability of clinical benefit after treatment discontinuation.
Results: Twenty-eight patients were enrolled of whom 27 were evaluable for efficacy. Patients received ibrutinib for a median of 21 months (range 7-67) prior to study enrollment. Fourteen patients (52%) have achieved U-MRD per protocol whereas 78% had at least one U-MRD evaluation. Seventeen patients (63%) have entered TFO after a median of 6.4 months on triplet therapy. Progression-free survival at 12 months was estimated at 95%. Grade ≥3 adverse events were hypertension 7%, diarrhea 4%, and increased ALT/AST 4%.
Conclusions: This triplet approach utilizes the addition of U2 to ibrutinib as an MRD-driven time-limited therapy. This therapy was well tolerated and effective. TFO following this therapy appears durable in ongoing follow-up.
©2022 American Association for Cancer Research.
Conflict of interest statement
Disclosure of Conflicts of Interest
LER has served as a consultant for AbbVie, Ascentage, AstraZeneca, Beigene, Janssen, Loxo Oncology, Nurix, Pharmacyclics, Pfizer, TG Therapeutics, served as a CME speaker for DAVA, Curio, and Medscape, holds minority ownership interest in Abbott Laboratories, received travel support from LOXO oncology, and has received research funding (paid to the institution) from Pfizer, Loxo Oncology, and Aptose Biosciences. LAL has served as an advisory board or panel participant, on speaker’s bureau and/or as a consultant for AbbVie, AstraZenca, BeiGene, Celgene/Bristol Myers Squibb, Epizyme, Karyopharm, Janssen, Kite/Gilead Sciences, Merck, Pharmacyclics, Seagen, TG Therapeutics. JDS has received consulting fees from Abbvie, AstraZeneca, Beigene, Biogen, Bristol Myers Squibb, Roche, TG Therapeutics, and Verastem, and research funding from Adaptive Biotechnologies, Beigene, BostonGene, Genentech/Roche, GlaxoSmithKline, MEI Pharma, Moderna, and TG Therapeutics. TAF served on speaker’s bureau for AbbVie, BMS, Celgene, Janssen Biotech, Pharmacyclics, Seattle Genetics, Takeda, and has served as a consultant for AbbVie, ADC Therapeutics, Astrazeneca, Daiichi Sakyo, Genmab, Karyopharm, KITE, MorphoSys. ADZ has served as a consultant for Genentech/Roche, Gilead, BMS/Celgene/JUNO, Janssen, Novartis, Adaptive Biotechnology, MorphoSys, Abbvie, AstraZeneca, MEI Pharma, BeiGene, received research funding from MEI Pharmaceuticals, Genentech/Roche, and Beigene, and was a DMC member for BMS/Celgene/Juno. LF has served as a consultant for Roche-Genentech, Genmab, AbbVie and ADC therapeutics, and has received research funding from Roche-Genentech and Genmab. JHP received advisory or consulting fees from Allogene, Amgen, Artiva, Autolus, BMS, Curocel, Incyte, InnatePharma, Kite Pharma, Kura Oncology, Minerva, Novartis, Pfizer, PrecisionBio, Servier and serves on a data monitoring committee for Affyimmune, BrightPharma, and Intellia. KB has served as a consultant for AbbVie. MCT has received honorarium from: MJH Life Sciences, Curio Science, VJHemOnc, Brazilian Association of Hematology and Hemotherapy (ABHH) and Massachusetts Medical Society. TT, MP, DP, HPM, PS are employed by TG therapeutics. ARM has served as a consultant for AbbVie, AstraZeneca, Beigene, Bristol Myers Squibb Company, Celgene, Genentech, Loxo Oncology, Octapharma, Pharmacyclics, Pfizer, TG Therapeutics, served as a CME speaker for DAVA, Curio, and Medscape, is a member of the medical advisory board for CLL Society and a scientific advisor for Lymphoma Research Foundation. All other authors declare no conflicts of interest.
Figures



References
-
- Munir T, Brown JR, O’Brien S, Barrientos JC, Barr PM, Reddy NM, et al. Final analysis from RESONATE: Up to six years of follow-up on ibrutinib in patients with previously treated chronic lymphocytic leukemia or small lymphocytic lymphoma. Am J Hematol 2019;94(12):1353–63 doi 10.1002/ajh.25638. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
