

Effectiveness of automated alerting system compared to usual care for the management of sepsis
- PMID: 35854120
- PMCID: PMC9296632
- DOI: 10.1038/s41746-022-00650-5
Effectiveness of automated alerting system compared to usual care for the management of sepsis
Abstract
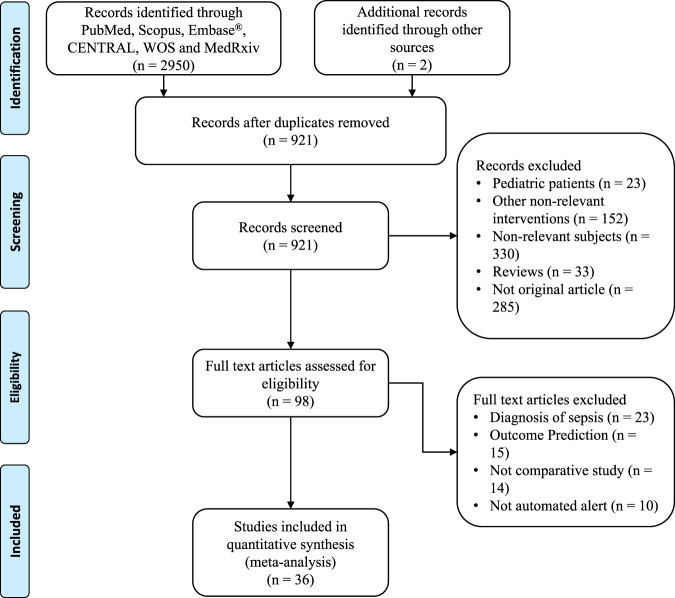
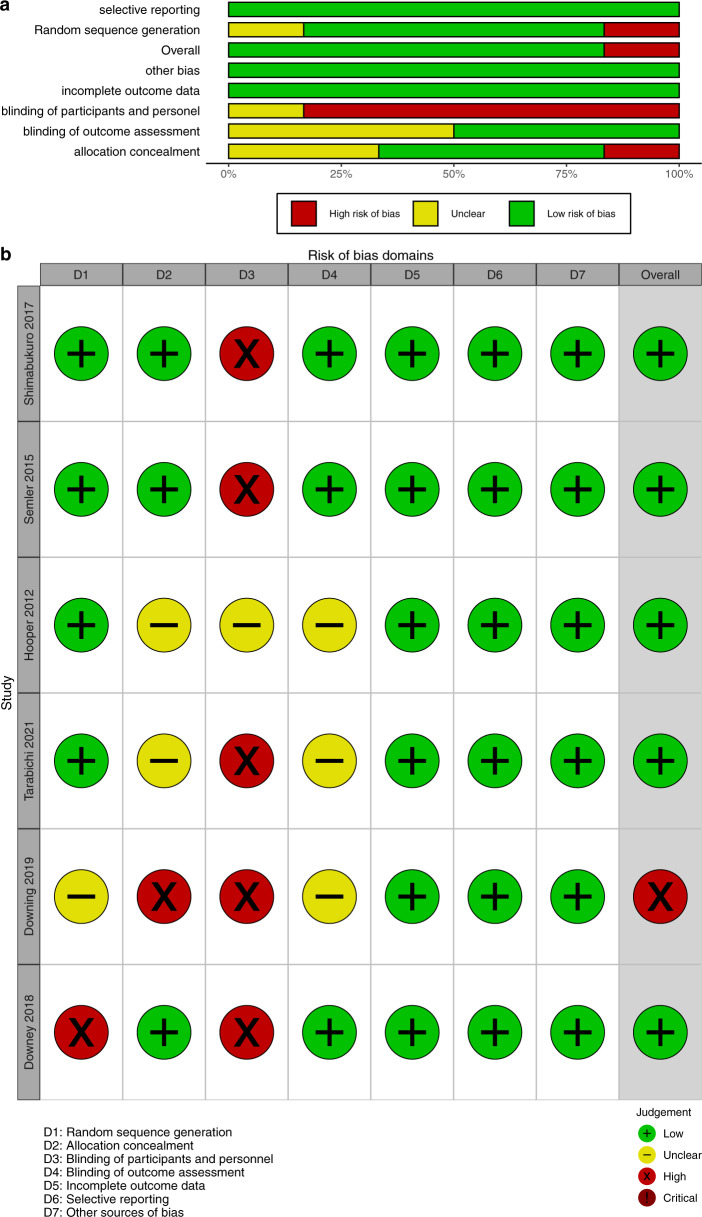
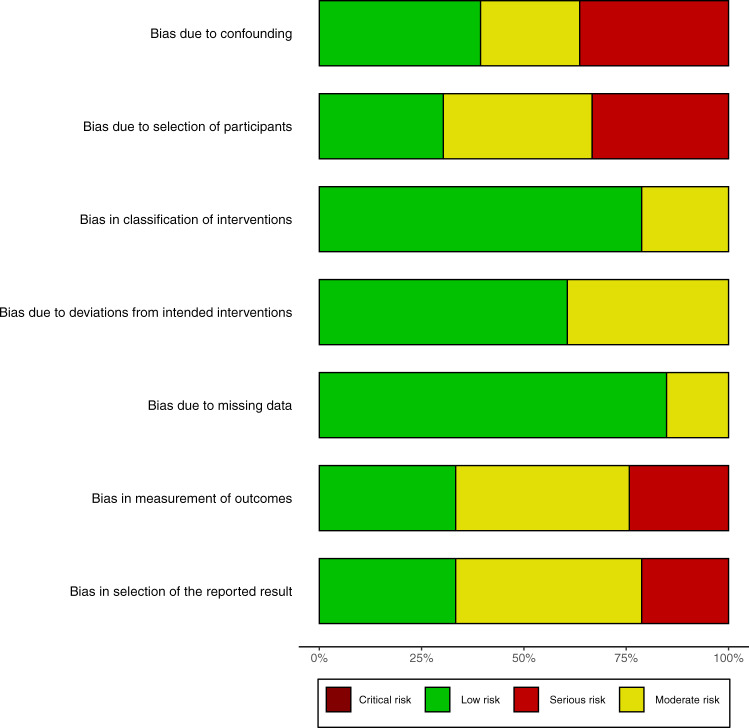
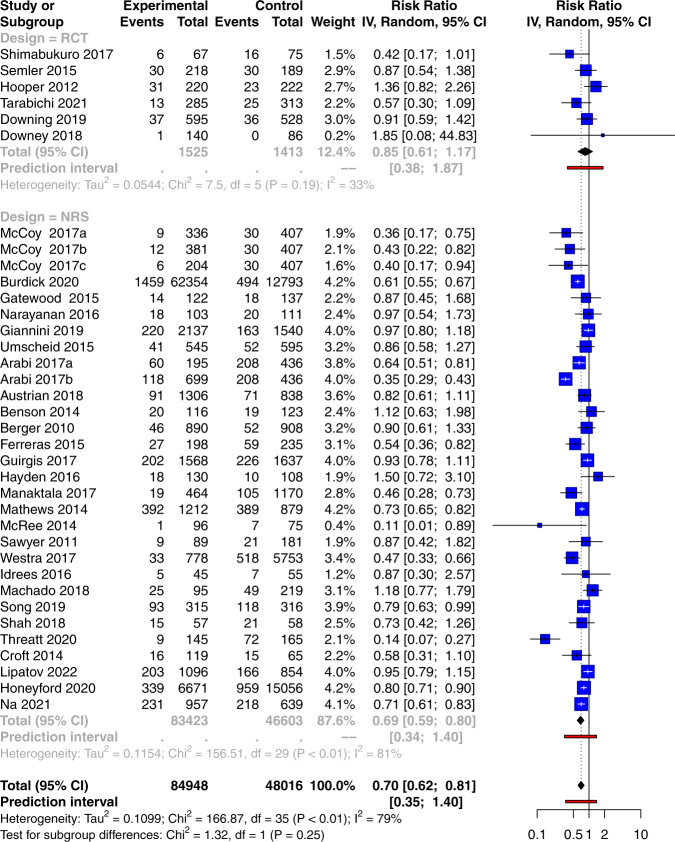
There is a large body of evidence showing that delayed initiation of sepsis bundle is associated with adverse clinical outcomes in patients with sepsis. However, it is controversial whether electronic automated alerts can help improve clinical outcomes of sepsis. Electronic databases are searched from inception to December 2021 for comparative effectiveness studies comparing automated alerts versus usual care for the management of sepsis. A total of 36 studies are eligible for analysis, including 6 randomized controlled trials and 30 non-randomized studies. There is significant heterogeneity in these studies concerning the study setting, design, and alerting methods. The Bayesian meta-analysis by using pooled effects of non-randomized studies as priors shows a beneficial effect of the alerting system (relative risk [RR]: 0.71; 95% credible interval: 0.62 to 0.81) in reducing mortality. The automated alerting system shows less beneficial effects in the intensive care unit (RR: 0.90; 95% CI: 0.73-1.11) than that in the emergency department (RR: 0.68; 95% CI: 0.51-0.90) and ward (RR: 0.71; 95% CI: 0.61-0.82). Furthermore, machine learning-based prediction methods can reduce mortality by a larger magnitude (RR: 0.56; 95% CI: 0.39-0.80) than rule-based methods (RR: 0.73; 95% CI: 0.63-0.85). The study shows a statistically significant beneficial effect of using the automated alerting system in the management of sepsis. Interestingly, machine learning monitoring systems coupled with better early interventions show promise, especially for patients outside of the intensive care unit.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
LinkOut - more resources
Full Text Sources
