

High coverage but low quality of maternal and newborn health services in the coverage cascade: who is benefitted and left behind in accessing better quality health services in Nepal?
- PMID: 35854265
- PMCID: PMC9297647
- DOI: 10.1186/s12978-022-01465-z
High coverage but low quality of maternal and newborn health services in the coverage cascade: who is benefitted and left behind in accessing better quality health services in Nepal?
Abstract
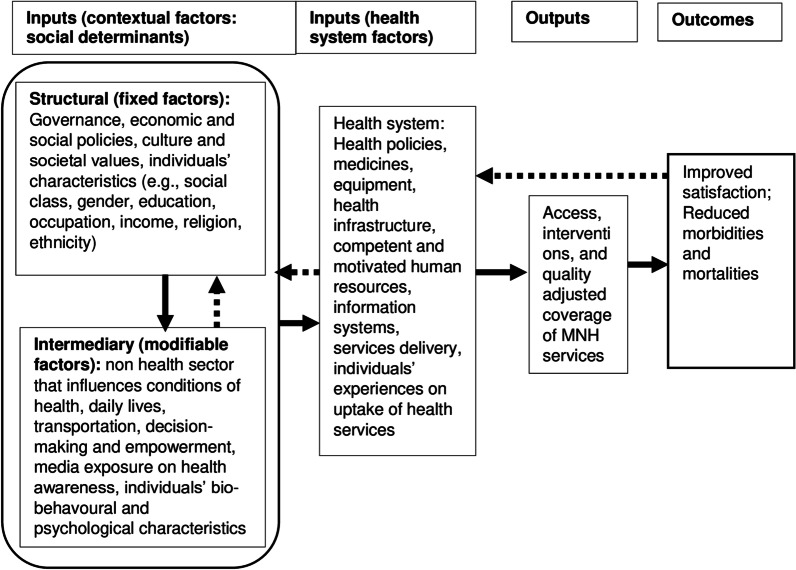
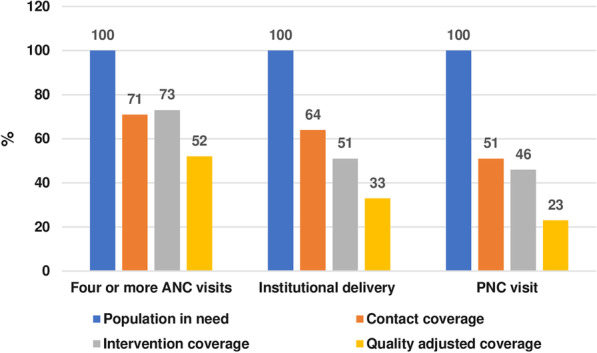
Background: Antenatal care (ANC) visits, institutional delivery, and postnatal care (PNC) visits are vital to improve the health of mothers and newborns. Despite improved access to these routine maternal and newborn health (MNH) services in Nepal, little is known about the cascade of health service coverage, particularly contact coverage, intervention-specific coverage, and quality-adjusted coverage of MNH services. This study examined the cascade of MNH services coverage, as well as social determinants associated with uptake of quality MNH services in Nepal.
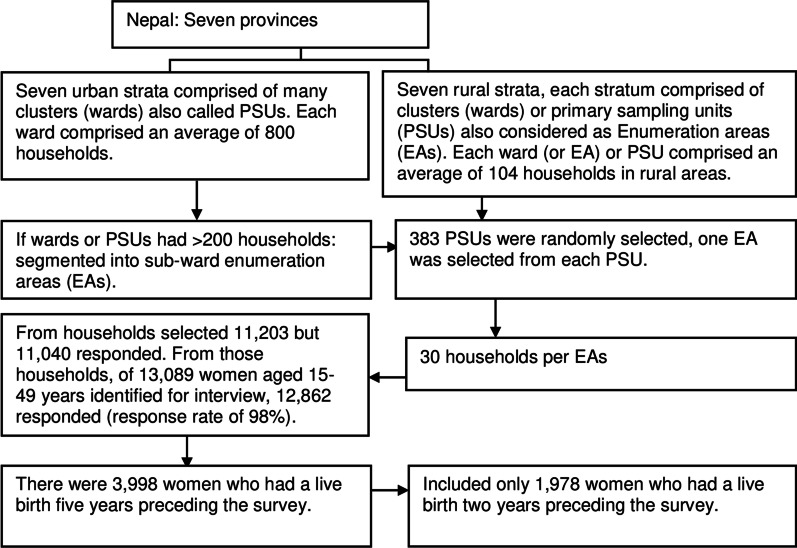
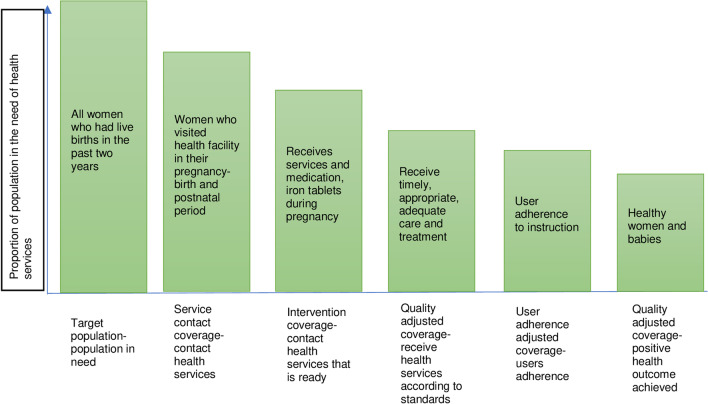
Methods: We conducted a secondary analysis of data derived from the Nepal Demographic and Health Survey (NDHS) 2016, taking 1978 women aged 15-49 years who had a live birth in the 2 years preceding the survey. Three outcome variables were (i) four or more (4+) ANC visits, (ii) institutional delivery, and (iii) first PNC visit for mothers and newborns within 48 h of childbirth. We applied a cascade of health services coverage, including contact coverage, intervention-specific and quality-adjusted coverage, using a list of specific intervention components for each outcome variable. Several social determinants of health were included as independent variables to identify determinants of uptake of quality MNH services. We generated a quality score for each outcome variable and dichotomised the scores into two categories of "poor" and "optimal" quality, considering > 0.8 as a cut-off point. Binomial logistic regression was conducted and odds ratios (OR) were reported with 95% confidence intervals (CIs) at the significance level of p < 0.05 (two-tailed).
Results: Contact coverage was higher than intervention-specific coverage and quality-adjusted coverage across all MNH services. Women with advantaged ethnicities or who had access to bank accounts had higher odds of receiving optimal quality MNH services, while women who speak the Maithili language and who had high birth order (≥ 4) had lower odds of receiving optimal quality ANC services. Women who received better quality ANC services had higher odds of receiving optimal quality institutional delivery. Women received poor quality PNC services if they were from remote provinces, had higher birth order and perceived problems when not having access to female providers.
Conclusions: Women experiencing ethnic and social disadvantages, and from remote provinces received poor quality MNH services. The quality-adjusted coverage can be estimated using household survey data, such as demographic and health surveys, especially in countries with limited routine data. Policies and programs should focus on increasing quality of MNH services and targeting disadvantaged populations and those living in remote areas. Ensuring access to female health providers and improving the quality of earlier maternity visits could improve the quality of health care during the pregnancy-delivery-postnatal period.
Keywords: Antenatal care; Coverage cascade; Determinants; Institutional delivery; Maternal and newborn health; Nepal; Postnatal care; Quality.
Plain language summary
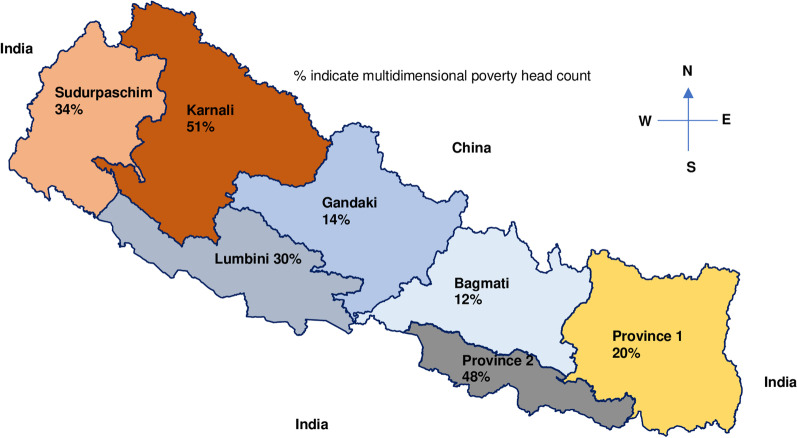
Utilisation of essential maternity and newborn health (MNH) interventions during pregnancy, childbirth, and the postnatal period can improve the health of mothers and newborns. There are increasing access trends for routine MNH visits in Nepal, such as at least four (4+) antenatal care (ANC) visits, institutional delivery, and postnatal care (PNC) visits. Little is known, however, about the utilisation of recommended MNH interventions, or who is benefitting or being left behind in relation to better quality MNH services. This study examined different types of health service coverage cascades across routine MNH services and associated determinants using Nepal Demographic and Health Survey 2016 data. A total of 1978 women aged 15–49 years who had live-births 2 years preceding the survey were included in the analysis. Despite improved access to routine visits during the pregnancy-postnatal period, some women had not received all recommended interventions, and had low-quality-adjusted coverage of MNH services. Women with advantaged ethnicities or financial assets received optimal quality MNH services, while Maithili-speaking women or those with high birth order received poor quality ANC services. Women from Karnali province or women who preferred to be seen by a female healthcare provider experienced poor quality PNC service. Demographic and health survey data can be used to assess the population-level coverage of quality health services. Policy and program efforts require better quality MNH services that employ female health providers.
© 2022. The Author(s).
Conflict of interest statement
The authors declared that they have no competing interests.
Figures
Similar articles
-
Universal coverage of the first antenatal care visit but poor continuity of care across the maternal and newborn health continuum among Nepalese women: analysis of levels and correlates.Global Health. 2021 Dec 11;17(1):141. doi: 10.1186/s12992-021-00791-4. Global Health. 2021. PMID: 34895276 Free PMC article.
-
Intersectional (in) equities in contact coverage of maternal and newborn health services in Nepal: insights from a nationwide cross-sectional household survey.BMC Public Health. 2021 Jun 9;21(1):1098. doi: 10.1186/s12889-021-11142-8. BMC Public Health. 2021. PMID: 34107922 Free PMC article.
-
Utilisation of quality antenatal, delivery and postnatal care services in Nepal: An analysis of Service Provision Assessment.Global Health. 2021 Sep 6;17(1):102. doi: 10.1186/s12992-021-00752-x. Global Health. 2021. PMID: 34488808 Free PMC article.
-
Trends of antenatal care during pregnancy in low- and middle-income countries: Findings from the global network maternal and newborn health registry.Semin Perinatol. 2019 Aug;43(5):297-307. doi: 10.1053/j.semperi.2019.03.020. Epub 2019 Mar 16. Semin Perinatol. 2019. PMID: 31005357 Free PMC article. Review.
-
Interventions to improve enablers and/or overcome barriers to seeking care during pregnancy, birthing and postnatal period for women living with vulnerabilities in high-income countries: A systematic review and meta-analysis.Midwifery. 2023 Jun;121:103674. doi: 10.1016/j.midw.2023.103674. Epub 2023 Mar 30. Midwifery. 2023. PMID: 37027983
Cited by
-
Investigating Health Inequality Using Trend, Decomposition and Spatial Analyses: A Study of Maternal Health Service Use in Nepal.Int J Public Health. 2023 Jun 2;68:1605457. doi: 10.3389/ijph.2023.1605457. eCollection 2023. Int J Public Health. 2023. PMID: 37332772 Free PMC article.
-
Continuum of care for maternal and newborn health services in Nepal: An analysis from demographic and health survey 2022.PLoS One. 2025 Mar 24;20(3):e0319033. doi: 10.1371/journal.pone.0319033. eCollection 2025. PLoS One. 2025. PMID: 40127091 Free PMC article.
-
Novel on-site follow-up and enhancement program (FEP) improves knowledge, clinical skills and enabling environment of skilled birth attendants in Nepal.PLoS One. 2023 Aug 22;18(8):e0285653. doi: 10.1371/journal.pone.0285653. eCollection 2023. PLoS One. 2023. PMID: 37607194 Free PMC article.
-
Contextual factors affecting the implementation of an anemia focused virtual counseling intervention for pregnant women in plains Nepal: a mixed methods process evaluation.BMC Public Health. 2023 Jul 6;23(1):1301. doi: 10.1186/s12889-023-16195-5. BMC Public Health. 2023. PMID: 37415262 Free PMC article. Clinical Trial.
-
Poor coverage of quality-adjusted antenatal care services: a population-level assessment by visit and source of antenatal care services in Bihar state of India.Lancet Reg Health Southeast Asia. 2023 Nov 28;25:100332. doi: 10.1016/j.lansea.2023.100332. eCollection 2024 Jun. Lancet Reg Health Southeast Asia. 2023. PMID: 39021484 Free PMC article.
References
-
- WHO . Trends in maternal mortality 2000 to 2017: estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division. Geneva: WHO; 2019.
-
- WHO . WHO recommendations on antenatal care for a positive pregnancy experience. Geneva: World Health Organization; 2016. - PubMed
-
- WHO . Compilation of WHO recommendations on maternal, newborn, child and adolescent health. Geneva: World Health Organization; 2013.
MeSH terms
LinkOut - more resources
Full Text Sources
