

Negative-pressure hydrocephalus in the course of a complex postoperative intracranial pressure disturbance: illustrative case
- PMID: 35854689
- PMCID: PMC9236168
- DOI: 10.3171/CASE206
Negative-pressure hydrocephalus in the course of a complex postoperative intracranial pressure disturbance: illustrative case
Abstract
Background: Negative-pressure hydrocephalus (NePH) is a rare clinical entity that presents on the background of ventriculomegaly with atypical symptoms. Its diagnosis is difficult, and some patients experience several shunt revisions until the proper solution is found.
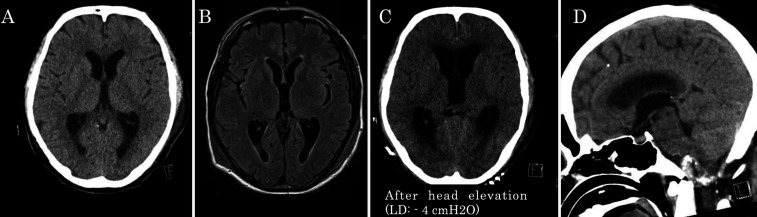
Observations: The authors present a patient who developed acute deterioration due to iatrogenic NePH after surgery for a vertebral artery thrombosed giant aneurysm. The deterioration occurred after the insertion of a lumbar drain by which the authors intended to reduce a postoperative subcutaneous cerebrospinal fluid (CSF) collection. The drainage created an unexpected negative-pressure gradient in the CSF spaces, which resulted in NePH. Interventions, such as extraventricular drainage and blood patch, corrected the negative transmantle pressure and stabilized the patient's condition.
Lessons: Because the pathophysiology of NePH is theoretically considered to be caused by negative transmantle pressure, the intervention should be performed in order to deal with the coexistence of obstruction in the CSF pathways and a CSF leak. A blood patch would be an effective option in treating the CSF leak when the site of leakage is certain. This is the first case in which a blood patch was effectively applied in the treatment for NePH with a favorable outcome without any permanent CSF diversion.
Keywords: CSAS = cortical subarachnoid space; CSF = cerebrospinal fluid; CT = computerized tomography; ETV = endoscopic third ventriculostomy; EVD = external ventricular drainage; GCS = Glasgow Coma Scale; MRI = magnetic resonance imaging; NePH = negative-pressure hydrocephalus; POD = postoperative day; VA = vertebral artery; blood patch; low-pressure hydrocephalus; negative-pressure hydrocephalus.
© 2021 The authors.
Conflict of interest statement
Disclosures The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.
Figures

Similar articles
-
A Rare Case of Negative-Pressure Hydrocephalus: A Plausible Explanation and the Role of Transmantle Theory.World Neurosurg. 2019 May;125:6-9. doi: 10.1016/j.wneu.2019.01.117. Epub 2019 Jan 31. World Neurosurg. 2019. PMID: 30710718
-
Syndrome of inappropriately low-pressure acute hydrocephalus (SILPAH).Acta Neurochir Suppl. 2012;113:155-9. doi: 10.1007/978-3-7091-0923-6_31. Acta Neurochir Suppl. 2012. PMID: 22116443
-
The pathophysiology of chronic noncommunicating hydrocephalus: lessons from continuous intracranial pressure monitoring and ventricular infusion testing.J Neurosurg. 2018 Jul;129(1):220-233. doi: 10.3171/2017.1.JNS162813. Epub 2017 Aug 11. J Neurosurg. 2018. PMID: 28799879
-
The importance of the cortical subarachnoid space in understanding hydrocephalus.J Neurosurg Pediatr. 2008 Jul;2(1):1-11. doi: 10.3171/PED/2008/2/7/001. J Neurosurg Pediatr. 2008. PMID: 18590387 Review.
-
Endoscopic third ventriculostomy and posterior fossa tumors.World Neurosurg. 2013 Feb;79(2 Suppl):S18.e15-9. doi: 10.1016/j.wneu.2012.02.018. Epub 2012 Feb 10. World Neurosurg. 2013. PMID: 22381845 Review.
References
-
- Filippidis AS, Kalani MY, Nakaji P, et al. Negative-pressure and low-pressure hydrocephalus: the role of cerebrospinal fluid leaks resulting from surgical approaches to the cranial base. J Neurosurg. 2011;115(5):1031–1037. - PubMed
-
- Strand A, Balise S, Leung LJ, et al. Low-pressure hydrocephalus: a case report and review of the literature. World Neurosurg. 2018;109:e131–e135. - PubMed
-
- Pang D, Altschuler E. Low-pressure hydrocephalic state and viscoelastic alterations in the brain. Neurosurgery. 1994;35(4):643–656. - PubMed
-
- Dias MS, Li V, Pollina J. Low-pressure shunt ‘malfunction’ following lumbar puncture in children with shunted obstructive hydrocephalus. Pediatr Neurosurg. 1999;30(3):146–150. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
