

Combined abnormalities of femoral version and acetabular version and McKibbin Index in FAI patients evaluated for hip preservation surgery
- PMID: 35854804
- PMCID: PMC9291377
- DOI: 10.1093/jhps/hnac016
Combined abnormalities of femoral version and acetabular version and McKibbin Index in FAI patients evaluated for hip preservation surgery
Abstract
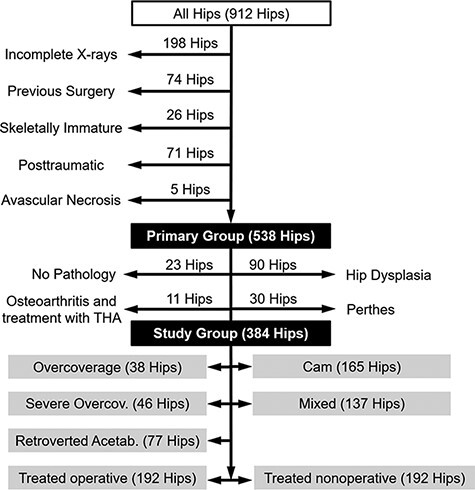
Frequencies of combined abnormalities of femoral version (FV) and acetabular version (AV) and of abnormalities of the McKibbin index are unknown. To investigate the prevalence of combined abnormalities of FV and AV and of abnormalities of the McKibbin index in symptomatic patients with femoroacetabular impingement (FAI), a retrospective, Institutional Review Board (IRB)-approved study of 333 symptomatic patients (384 hips) that were presented with hip pain and FAI was performed. The computed tomography/magnetic resonance imaging based measurement of central AV, cranial AV and FV was compared among five subgroups with distinguished FAI subgroups and patients that underwent a hip preservation surgery. The allocation to each subgroup was based on AP radiographs. Normal AV and FV were 10-25°. The McKibbin index is the sum of central AV and FV. Of patients that underwent a hip preservation surgery, 73% had a normal McKibbin index (20-50°) but 27% had an abnormal McKibbin index. Of all patients, 72% had a normal McKibbin index, but 28% had abnormal McKibbin index. The prevalence of combined abnormalities of FV and AV varied among subgroups: a higher prevalence of decreased central AV combined with decreased FV of patients with acetabular-retroversion group (12%) and overcoverage (11%) was found compared with mixed-type FAI (5%). Normal AV combined with normal FV was present in 41% of patients with cam-type FAI and in 34% of patients with overcoverage. Patients that underwent a hip preservation surgery had normal mean FV (17 ± 11°), central AV (19 ± 7°), cranial AV (16 ± 10°) and McKibbin index (36 ± 14°). Frequency of combined abnormalities of AV and FV differs between subgroups of FAI patients. Aggravated and compensated McKibbin index was prevalent in FAI patients. This has implications for open hip preservation surgery (surgical hip dislocation or femoral derotation osteotomy) or hip arthroscopy or non-operative treatment.
© The Author(s) 2022. Published by Oxford University Press.
Figures




References
-
- Chadayammuri V, Garabekyan T, Bedi A et al. Passive hip range of motion predicts femoral torsion and acetabular version. J Bone Joint Surg Am 2016; 98: 127–34. - PubMed
-
- Lerch TD, Boschung A, Todorski IAS et al. Femoroacetabular impingement patients with decreased femoral version have different impingement locations and intra- and extraarticular anterior subspine FAI on 3D-CT-based impingement simulation: implications for hip arthroscopy. Am J Sports Med 2019; 47: 3120–32. doi: 10.1177/0363546519873666 - DOI - PubMed
-
- Tönnis D, Heinecke A. Acetabular and femoral anteversion: relationship with osteoarthritis of the hip. J Bone Joint Surg Am 1999; 81: 1747–70. - PubMed
