

Occipitocervical fusion of traumatic atlanto-occipital dissociation in a patient with autofused cervical facet joints: illustrative case
- PMID: 35854957
- PMCID: PMC9272367
- DOI: 10.3171/CASE21276
Occipitocervical fusion of traumatic atlanto-occipital dissociation in a patient with autofused cervical facet joints: illustrative case
Abstract
Background: Patients who survive traumatic atlanto-occipital dissociation (AOD) may present with normal neurological examinations and near-normal-appearing diagnostic images, such as cervical radiographs and computed tomography (CT) scans.
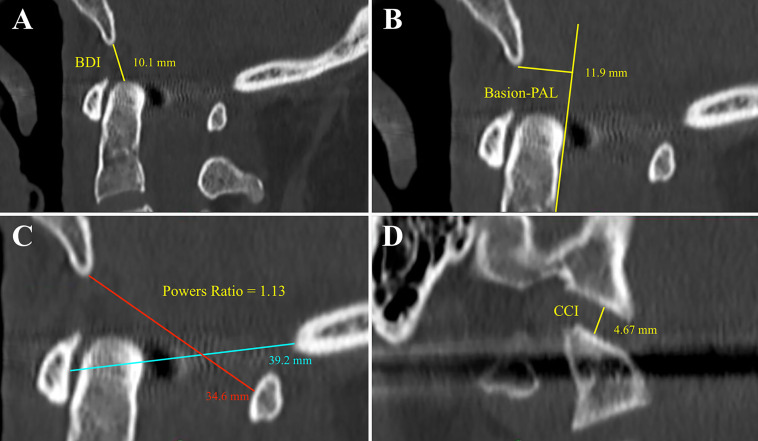
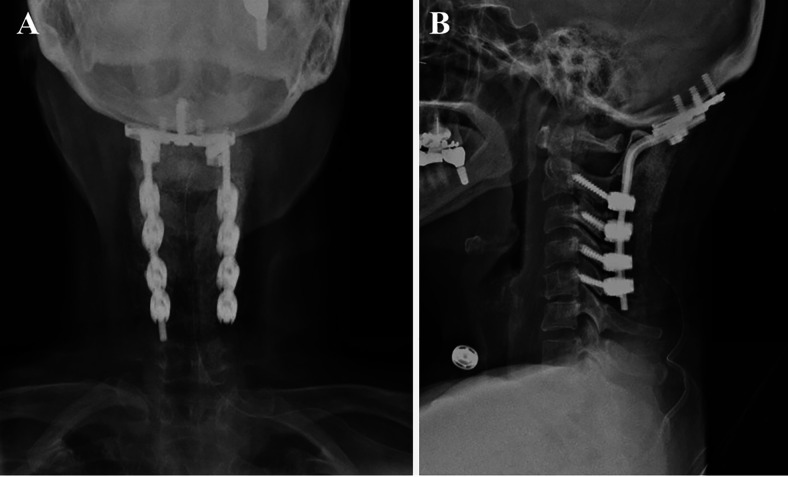
Observations: The authors described a neurologically intact 64-year-old female patient with a degenerative autofusion of her right C4-5 facet joints who presented to their center after a motor vehicle collision. Prevertebral soft tissue swelling and craniocervical subarachnoid hemorrhage prompted awareness and consideration for traumatic AOD. An abnormal occipital condyle-C1 interval (4.67 mm) on CT and craniocervical junction ligamentous injury on magnetic resonance imaging (MRI) confirmed the diagnosis of AOD. Her autofused right C4-5 facet joints were incorporated into the occipitocervical fusion construct.
Lessons: Traumatic AOD can be easily overlooked in patients with a normal neurological examination and no associated upper cervical spine fractures. A high index of suspicion is needed when evaluating CT scans because normal values for craniocervical parameters are significantly different from the accepted ranges of normal on radiographs in the adult population. MRI of the cervical spine is helpful to evaluate for atlanto-occipital ligamentous injury and confirm the diagnosis. Occipitocervical fusion construct may need to be extended to incorporate spinal levels with degenerative autofusion to prevent adjacent level degeneration.
Keywords: AOD = atlanto-occipital dissociation; BAI = basion-axial interval; BDI = basion-dens interval; CCI = condyle–C1 interval; CT = computed tomography; MRI = magnetic resonance imaging; PAL = posterior axial line; STIR = short tau inversion recovery; atlanto-occipital dislocation; atlanto-occipital dissociation; degenerative facet fusion; facet joint autofusion; occipitocervical fusion.
© 2021 The authors.
Conflict of interest statement
Disclosures The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.
Figures



References
-
- Mendenhall SK, Sivaganesan A, Mistry A, et al. Traumatic atlantooccipital dislocation: comprehensive assessment of mortality, neurologic improvement, and patient-reported outcomes at a Level 1 trauma center over 15 years. Spine J. 2015;15(11):2385–2395. - PubMed
-
- Theodore N, Aarabi B, Dhall SS, et al. The diagnosis and management of traumatic atlanto-occipital dislocation injuries. Neurosurgery. 2013;72(suppl 2):114–126. - PubMed
-
- Liao S, Jung MK, Hörnig L, et al. Injuries of the upper cervical spine: how can instability be identified? Int Orthop. 2020;44(7):1239–1253. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
