

Identification of Streptomyces spp. in a Clinical Sample: Always Contamination? Results of a French Retrospective Study
- PMID: 35854995
- PMCID: PMC9290580
- DOI: 10.1093/ofid/ofac271
Identification of Streptomyces spp. in a Clinical Sample: Always Contamination? Results of a French Retrospective Study
Abstract
Background: Streptomyces are environmental gram-positive bacilli that can cause ubiquitous mycetoma and, more rarely, invasive infections. We describe the clinical relevance of Streptomyces spp. identified in human samples and characteristics of patients with invasive Streptomyces infections.
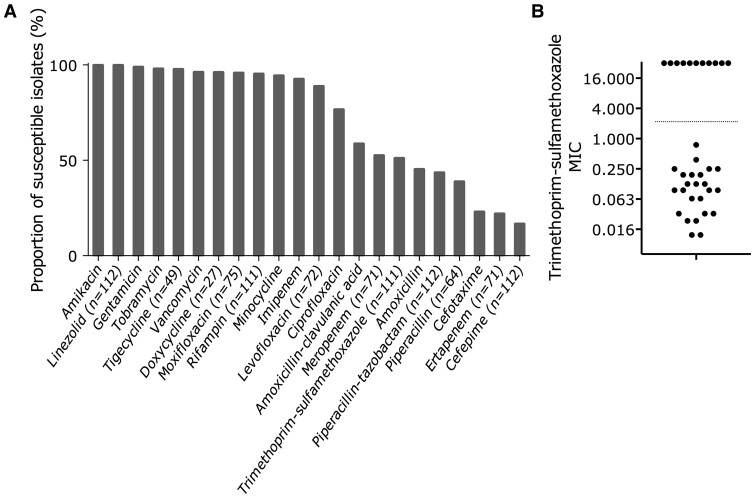
Methods: We conducted a retrospective (2006-2017) study of Streptomyces isolates identified in clinical samples in French microbiology laboratories. Streptomyces genus was confirmed by a specific 16S rRNA polymerase chain reaction, and antibiotic susceptibility testing was performed by disk diffusion and trimethoprim-sulfamethoxazole minimum inhibitory concentration (E-test) if resistance was suspected. Patient characteristics, treatments, and outcomes were collected. Invasive infection was defined as a positive culture from a sterile site with signs of infection but without cutaneous inoculation.
Results: Of 137 Streptomyces isolates, all were susceptible to amikacin (113/113) and linezolid (112/112), and 92.9% to imipenem (105/113). Using disk diffusion, 50.9% (57/112) of isolates were susceptible to trimethoprim-sulfamethoxazole, but most of the apparently resistant isolates (25/36, 69.4%) tested by E-test were ultimately classified as susceptible. Clinical data were obtained for 63/137 (45.9%) isolates: 30 (47.6%) invasive infections, 8 (12.7%) primary cutaneous infections, 22 (34.9%) contaminations, 3 (4.7%) respiratory colonization. Patients with invasive infection were more frequently receiving corticosteroids than patients without invasive infection (11/30, 36.7%, vs 2/25, 8.0%; P = .03), and at 6-month follow-up, 14 of them were cured, 3 had relapsed, 4 were dead, and 9 were lost to follow-up.
Conclusions: Half of the clinical samples that grew Streptomyces were from patients with invasive infection. In that case, antimicrobial therapy should include 1 or 2 antibiotics among linezolid, amikacin, or imipenem.
Keywords: Actinobacteria; contamination; environment; invasive infection.
© The Author(s) 2022. Published by Oxford University Press on behalf of the Infectious Diseases Society of America.
Figures

References
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Miscellaneous
