

Fatal ruptured occult arteriovenous malformation in a young adult: An autopsy case report
- PMID: 35855123
- PMCID: PMC9282792
- DOI: 10.25259/SNI_427_2022
Fatal ruptured occult arteriovenous malformation in a young adult: An autopsy case report
Abstract
Background: Brain arteriovenous malformations (AVMs) are congenital developmental disorders with unclear causative factors and pathogenic mechanisms. Various epigenetic factors may influence the development and rupture of AVMs. Ruptured AVMs may lead to poor outcomes. Therefore, the risk factors of AVM rupture and treatment strategies for unruptured AVMs should be explored. Herein, we report a case of a fatal ruptured AVM diagnosed by radiological and autopsy findings and review the literature regarding AVM treatment.
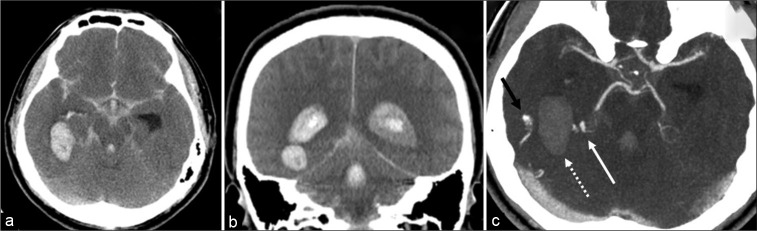
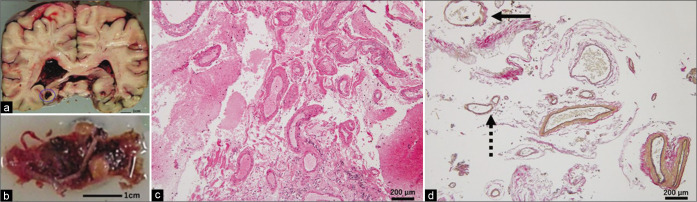
Case description: A 46-year-old man was brought to the hospital with sudden loss of consciousness while sitting on the edge of the bathtub. On examination, he was unconscious with poor breathing efforts. He was intubated and a brain CT scan was performed, which showed an intracerebral hemorrhage (ICH) adjacent to the right trigone with massive intraventricular hemorrhage (IVH) and subarachnoid hemorrhage (SAH). Contrast-enhanced CT scan showed abnormal vessels adjacent to the hematoma. He was diagnosed with ICH associated with IVH and SAH caused by a ruptured abnormal vascular lesion. He underwent external ventricular drainage to control the intracranial pressure. He remained unconscious and died 16 h after hospital admission. Autopsy was performed to identify the cause of ICH. Pathological sections showed a mass of blood vessels, measuring 20 × 10 × 10 mm in size, within the hematoma with a single drainer connecting to the transverse sinus. These blood vessels had variable size, shape, and wall thickness on microscopy. Some vessels had abnormal thickened walls with discontinuous elastic fibers. Based on the radiological and autopsy findings, an ICH secondary to SpetzlerMartin Grade I AVM was confirmed.
Conclusion: If the cause of ICH cannot be determined during a patient's life, autopsy may be performed to determine the pathophysiology of occult vascular lesions, including AVMs. Patients with AVMs may have moderate or no symptoms before and after rupture. Because deep AVMs fed by posterior circulation have high risk of bleeding, surgical intervention should be considered for these patients to prevent a poor outcome. Low-grade and paraventricular AVMs in a young adult may be successfully treated with multimodal surgery.
Keywords: Diagnostic imaging; Endovascular procedures; Hemorrhagic stroke; Intracranial arteriovenous malformation; Microsurgery.
Copyright: © 2022 Surgical Neurology International.
Conflict of interest statement
There are no conflicts of interest.
Figures
Similar articles
-
International multicenter cohort study of pediatric brain arteriovenous malformations. Part 2: Outcomes after stereotactic radiosurgery.J Neurosurg Pediatr. 2017 Feb;19(2):136-148. doi: 10.3171/2016.9.PEDS16284. Epub 2016 Dec 2. J Neurosurg Pediatr. 2017. PMID: 27911249
-
Spontaneous subdural hematoma concomitant with subarachnoid hemorrhage and intracerebral hemorrhage due to ruptured brain arteriovenous malformation treated with curative embolization.J Neurosci Rural Pract. 2023 Apr-Jun;14(2):368-370. doi: 10.25259/JNRP_13_2023. Epub 2023 Apr 5. J Neurosci Rural Pract. 2023. PMID: 37181178 Free PMC article.
-
Effect of prior hemorrhage on intracranial arteriovenous malformation radiosurgery outcomes.Cerebrovasc Dis. 2015;39(1):53-62. doi: 10.1159/000369959. Epub 2014 Dec 24. Cerebrovasc Dis. 2015. PMID: 25547253
-
Ruptured Distal Posterior Inferior Cerebellar Artery (PICA) Aneurysms Associated with Cerebellar Arterial Venous Malformations (AVMs): A Case Series and Review of the Literature Demonstrating the Need for Angiographic Evaluation and Feasibility of Endovascular Treatment.World Neurosurg. 2017 Jan;97:751.e7-751.e13. doi: 10.1016/j.wneu.2016.10.081. Epub 2016 Oct 25. World Neurosurg. 2017. PMID: 27793767 Review.
-
The natural history of cerebral arteriovenous malformations.Handb Clin Neurol. 2017;143:15-24. doi: 10.1016/B978-0-444-63640-9.00002-3. Handb Clin Neurol. 2017. PMID: 28552137 Review.
References
-
- Alén JF, Lagares A, Paredes I, Campollo J, Navia P, Ramos A, et al. Cerebral microarteriovenous malformations: A series of 28 cases. J Neurosurg. 2013;119:594–602. - PubMed
-
- Amin-Hanjani S. ARUBA results are not applicable to all patients with arteriovenous malformation. Stroke. 2014;45:1539–40. - PubMed
-
- Batjer H, Samson D. Surgical approaches to trigonal arteriovenous malformations. J Neurosurg. 1987;67:511–7. - PubMed
-
- de Castro-Afonso LH, Vanzim JR, Trivelato FP, Rezende MT, Ulhôa AC, Chodraui-Filho SF, et al. Association between draining vein diameters and intracranial arteriovenous malformation hemorrhage: A multicentric retrospective study. Neuroradiology. 2020;62:1497–505. - PubMed
-
- Ding D, Starke RM, Kano H, Mathieu D, Huang P, Kondziolka D, et al. Radiosurgery for cerebral arteriovenous malformations in a randomized trial of unruptured brain arteriovenous malformations (ARUBA)-eligible patients: A multicenter study. Stroke. 2016;47:342–9. - PubMed
Publication types
LinkOut - more resources
Full Text Sources