

Pros of the contralateral (over-the-top) approach to intra/extraforaminal lumbar disc herniations at the L5-S1 level
- PMID: 35855125
- PMCID: PMC9282753
- DOI: 10.25259/SNI_400_2022
Pros of the contralateral (over-the-top) approach to intra/extraforaminal lumbar disc herniations at the L5-S1 level
Abstract
Background: Minimally invasive approaches to intra/extraforaminal lumbar disc herniations offer the benefit of less bone removal and reduced nerve root manipulation at the L5-S1 level. Moreover, the potential to better preserve stability.
Methods: Here, we summarized the efficacy of the contralateral approach to intraforaminal/extraforaminal lumbar disc herniations particularly focusing on the L5-S1 level. Variables studied included the level of these disc herniations, their locations within the foramina, and the anatomy of the facet joints.
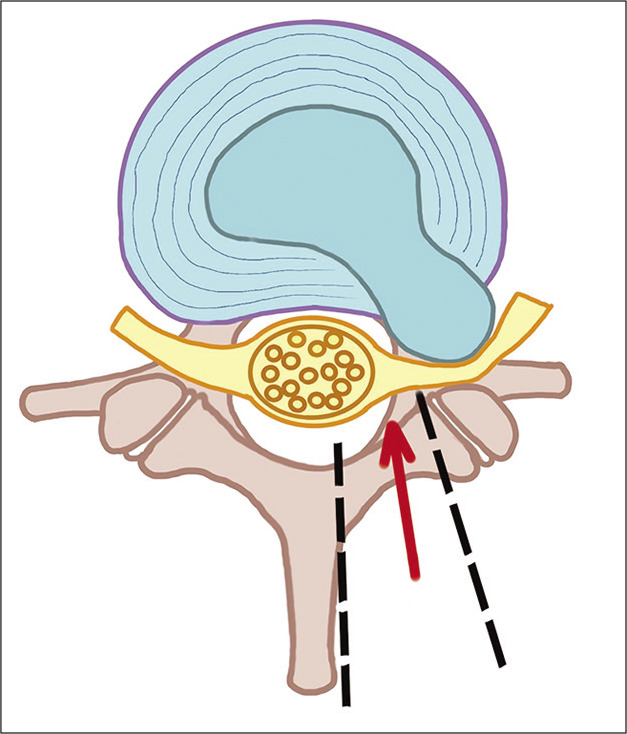
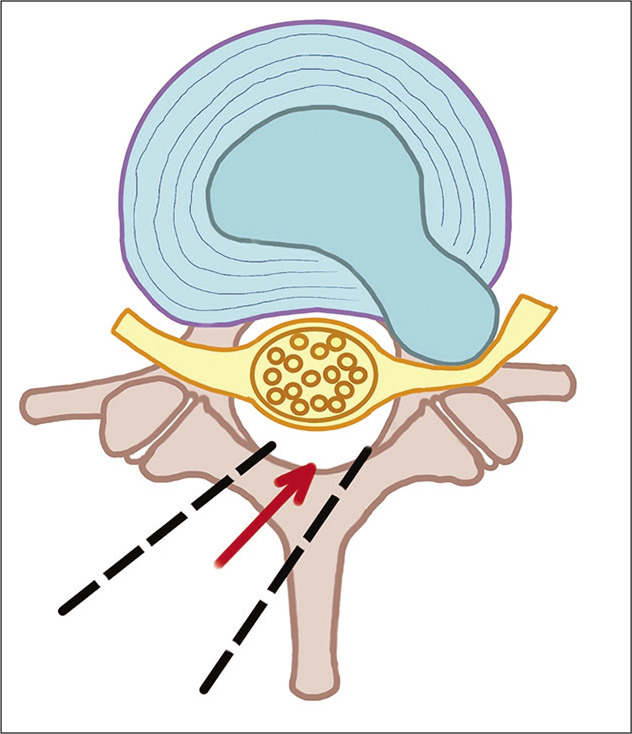
Results: A major "pro" for the contralateral interlaminar procedure at the L5-S1 level is that it does not require facet joint removal, or with a spondylotic facet, <30% joint excision, to directly visualize the intraforaminal/ extraforaminal nerve root. It, therefore, reduces the risk of creating iatrogenic instability, while offering a higher certitude of adequate nerve root visualization, decompression, and safer disc removal.
Conclusion: The contralateral interlaminar approach is more suitable for all types of intra/extraforaminal disc herniations at the L5/S1 level. The most specific benefit of this approach is its avoidance of disruption/significant removal (i.e., <30%) of the facet joint to adequately expose the foraminal L5 nerve root, and more safely remove the intra/extraforaminal disc herniation.
Keywords: Contralateral approach; Crossover technique; Intraforaminal lumbar disc herniation; Minimally invasive spine surgery; Over-the-top access; Spinal stability.
Copyright: © 2022 Surgical Neurology International.
Conflict of interest statement
There are no conflicts of interest.
Figures
Similar articles
-
A minimally invasive transmuscular approach to far-lateral L5-S1 level disc herniations: a prospective study.J Spinal Disord Tech. 2007 Apr;20(2):132-8. doi: 10.1097/01.bsd.0000211268.43744.2a. J Spinal Disord Tech. 2007. PMID: 17414982 Clinical Trial.
-
Contralateral interlaminar approach for intraforaminal lumbar degenerative disease with special emphasis on L5-S1 level: A technical note.Surg Neurol Int. 2016 Sep 21;7:88. doi: 10.4103/2152-7806.191024. eCollection 2016. Surg Neurol Int. 2016. PMID: 27713854 Free PMC article.
-
The Contralateral Approach to intra- and Extraforaminal Lumbar Disk Herniations: Surgical Technique and Review of Surgical Procedures.J Neurol Surg A Cent Eur Neurosurg. 2022 Nov;83(6):511-515. doi: 10.1055/s-0041-1739221. Epub 2021 Dec 12. J Neurol Surg A Cent Eur Neurosurg. 2022. PMID: 34897627 Review.
-
Percutaneous Endoscopic Transforaminal Outside-In Outside Technique for Foraminal and Extraforaminal Lumbar Disc Herniations-Operative Technique.World Neurosurg. 2019 Oct;130:244-253. doi: 10.1016/j.wneu.2019.07.005. Epub 2019 Jul 9. World Neurosurg. 2019. PMID: 31299304
-
Minimally invasive far lateral microendoscopic discectomy for extraforaminal disc herniation at the lumbosacral junction: cadaveric dissection and technical case report.Spine J. 2007 Jul-Aug;7(4):414-21. doi: 10.1016/j.spinee.2006.07.008. Epub 2007 Jan 30. Spine J. 2007. PMID: 17630139 Review.
References
-
- Abdullah AF, Wolber PG, Warfield JR, Gunadi IK. Surgical management of extreme lateral lumbar disc herniations: Review of 138 cases. Neurosurgery. 1988;22:648–53. - PubMed
-
- Berra LV, Foti D, Ampollini A, Faraca G, Zullo N, Musso C. Contralateral approach for far lateral lumbar disc herniations: A modified technique and outcome analysis of nine patients. Spine (Phila Pa 1976) 2010;35:709–13. - PubMed
-
- Epstein NE. Evaluation of varied surgical approaches used in the management of 170 far-lateral lumbar disc herniations: Indications and results. J Neurosurg. 1995;83:648–56. - PubMed
-
- Hodges SD, Humphreys SC, Eck JC, Covington LA. The surgical treatment of far lateral L3-L4 and L4-L5 disc herniations. A modified technique and outcomes analysis of 25 patients. Spine (Phila Pa 1976) 1999;24:1243–6. - PubMed
-
- Kunogi J, Hasue M. Diagnosis and operative treatment of intraforaminal and extraforaminal nerve root compression. Spine (Phila Pa 1976) 1991;16:1312–20. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous