

Cerebellopontine angle metastasis of a neuroendocrine tumor mimicking vestibular schwannoma: A case report
- PMID: 35855178
- PMCID: PMC9282763
- DOI: 10.25259/SNI_117_2022
Cerebellopontine angle metastasis of a neuroendocrine tumor mimicking vestibular schwannoma: A case report
Abstract
Background: Neuroendocrine tumors (NETs) are uncommon neoplasms arising from neuroendocrine cells and are rarely associated with intracranial metastases.
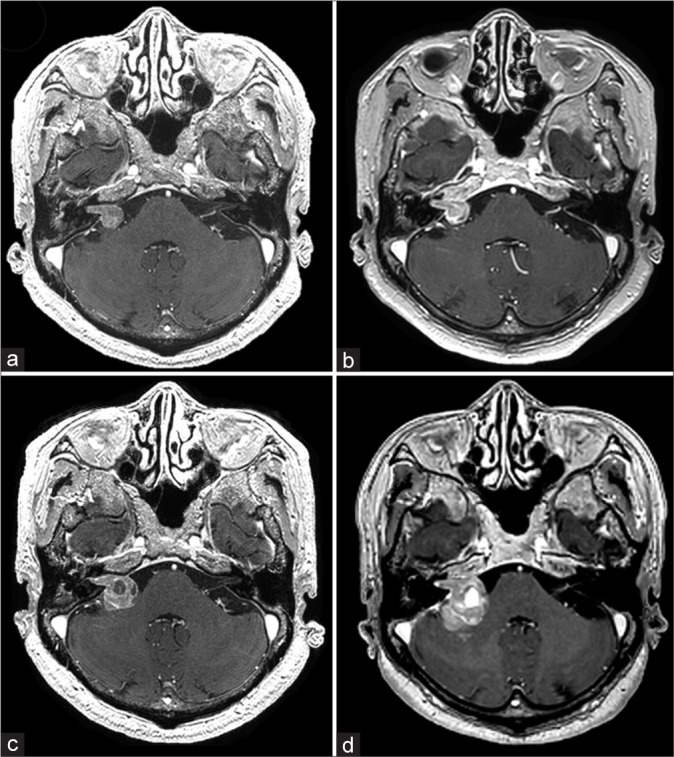
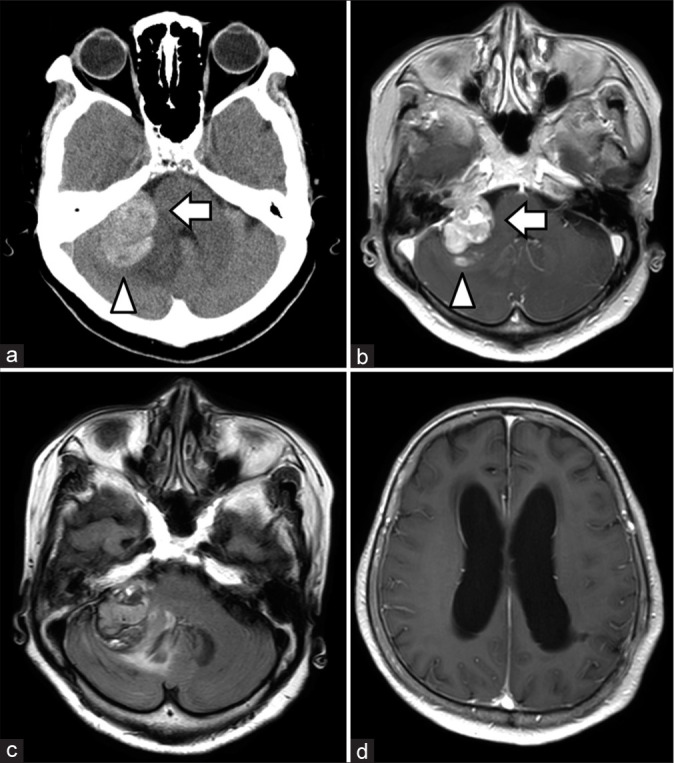
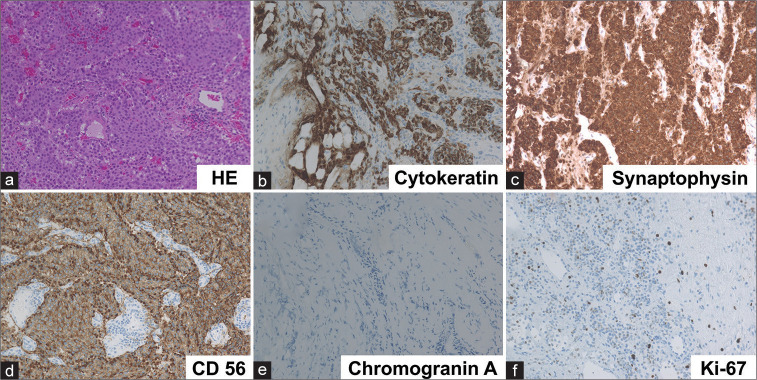
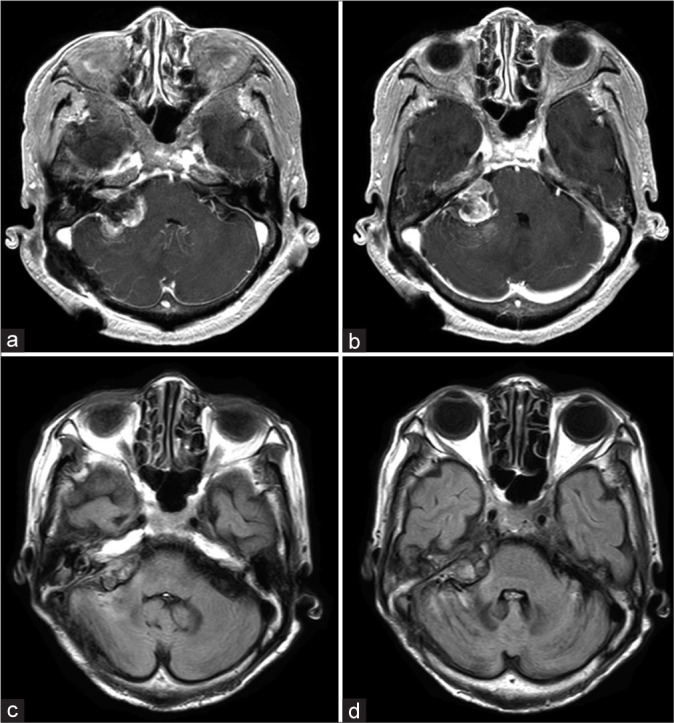
Case description: We discuss the case of a 74-year-old woman with a right CPA tumor. She had a history of retroperitoneal NET, but was diagnosed with vestibular schwannoma due to a right-sided hearing loss and a right CPA tumor along the VII and VIII nerves. After a 3-year follow-up, she presented with repetitive vomiting, a 1-month history of gait instability, and a 3-month history of general fatigue. Brain imaging revealed tumor growth and edematous changes in the right cerebellum. She underwent retrosigmoid craniotomy and partial resection. Histopathological examination revealed metastatic NET. She underwent stereotactic radiosurgery for residual lesion and, at 11 months of follow-up, the lesion was confirmed to have shrunk on magnetic resonance imaging (MRI).
Conclusion: This is the first case to report the natural course of cerebellopontine metastasis of a NET. The differential diagnosis of CPA tumors is diverse, and, in our case, we suspected a vestibular schwannoma because of the typical symptoms and imaging features. However, the tumor grew relatively faster than expected and showed intratumoral hemorrhage during the 3-year follow-up. Therefore, in patients with a history of a NET, a careful follow-up is advisable even for lesions highly suspected to be another benign tumor on MRI. Careful follow-up imaging and appropriate treatment strategies were useful to manage the brain metastasis. Although NETs metastasizing to the CPA are extremely rare, this possibility should be considered when patients with NETs have intracranial lesions.
Keywords: Brain metastasis; Case report; Cerebellopontine angle tumor; Neuroendocrine tumor; Neuroendocrine tumors; Vestibular schwannoma.
Copyright: © 2022 Surgical Neurology International.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Brown PD, Ballman KV, Cerhan JH, Anderson SK, Carrero XW, Whitton AC, et al. Postoperative stereotactic radiosurgery compared with whole brain radiotherapy for resected metastatic brain disease (NCCTG N107C/CEC·3): A multicentre, randomised, controlled, phase 3 trial. Lancet Oncol. 2017;18:1049–60. - PMC - PubMed
-
- Harrison CJ, Martin SC, Hofer M, Corkill R, Jeyaretna DS, Griffiths SJ. More than meets the MRI: Case report of a carcinoid tumour metastasis mimicking a meningioma. Br J Neurosurg. 2019;33:229–30. - PubMed
-
- Hlatky R, Suki D, Sawaya R. Carcinoid metastasis to the brain. Cancer. 2004;101:2605–13. - PubMed
Publication types
LinkOut - more resources
Full Text Sources