

Postoperative Lemierre's syndrome: a previously unreported complication of transoral surgery. Illustrative case
- PMID: 35855218
- PMCID: PMC9245783
- DOI: 10.3171/CASE20118
Postoperative Lemierre's syndrome: a previously unreported complication of transoral surgery. Illustrative case
Abstract
Background: Lemierre's syndrome is a rare but potentially life-threatening clinical condition characterized by bacteremia and thrombophlebitis of the internal jugular vein, usually secondary to oropharyngeal infection and often caused by Fusobacterium necrophorum; rarely, it occurs after surgical procedures. The most common clinical presentation includes acute pharyngitis, high fever, and neck pain. The diagnosis is based on blood culture and cranial and cervical spine computed tomography (CT)/magnetic resonance imaging (MRI) with contrast. Antibiotic therapy for 3-6 weeks is the mainstay of treatment, while the use of anticoagulant drugs is controversial.
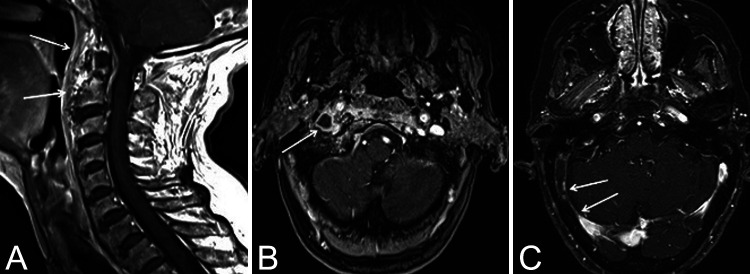
Observations: The authors describe a case of Lemierre's syndrome that occurred after transoral surgery. The patient underwent a combined surgical approach from above (transoral) and below (anterolateral transcervical) to the upper cervical spine for the resection of a large anterior osteophyte causing dysphagia, globus sensation, and dysphonia. Three weeks after the surgical procedure, she developed fever and severe neck pain.
Lessons: The aim of this paper is to consider Lemierre's syndrome as a possible complication after the transoral approach, underlining the importance of its early diagnosis and with a suggestion to perform cranial and cervical spine CT or MRI venous angiography in patients who undergo surgery with a transoral approach and exhibit local or systemic signs of infection such as neck pain, persistent fever, and positive blood culture results.
Keywords: CT = computed tomography; ENT = ear, nose, and throat; IJV = internal jugular vein; LS = Lemierre’s syndrome; Lemierre’s syndrome; MRI = magnetic resonance imaging; POD = postoperative day; WBC = white blood cell; cervical osteophyte; transoral approach.
© 2021 The authors.
Conflict of interest statement
Disclosures The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.
Figures




Similar articles
-
Lemierre's syndrome secondary to community-acquired methicillin-resistant Staphylococcus aureus infection presenting with cardiac tamponade, a rare disease with a life-threatening presentation: a case report.Int J Emerg Med. 2014 Sep 26;7:39. doi: 10.1186/s12245-014-0039-y. eCollection 2014. Int J Emerg Med. 2014. PMID: 25635199 Free PMC article.
-
High risk and low prevalence diseases: Lemierre's syndrome.Am J Emerg Med. 2022 Nov;61:98-104. doi: 10.1016/j.ajem.2022.08.050. Epub 2022 Aug 30. Am J Emerg Med. 2022. PMID: 36058204 Review.
-
Middle Ear Cholesteatoma Complicated By Lemierre's Syndrome: A Case Report and Literature Review.Ear Nose Throat J. 2025 Feb 28:1455613251323992. doi: 10.1177/01455613251323992. Online ahead of print. Ear Nose Throat J. 2025. PMID: 40018750
-
Case report: The use of metagenomic next-generation sequencing to diagnose Lemierre's syndrome caused by lost root canal fillings in a 33-year-old patient with metabolic syndrome.Front Med (Lausanne). 2024 Aug 14;11:1402444. doi: 10.3389/fmed.2024.1402444. eCollection 2024. Front Med (Lausanne). 2024. PMID: 39206169 Free PMC article.
-
Lemierre's syndrome: A forgotten and re-emerging infection.J Microbiol Immunol Infect. 2020 Aug;53(4):513-517. doi: 10.1016/j.jmii.2020.03.027. Epub 2020 Apr 4. J Microbiol Immunol Infect. 2020. PMID: 32303484 Review.
References
-
- Lemierre A. On certain septicæmias due to anaerobic organisms. Lancet. 1936;1:701–703.
-
- Hong P, MacCormick J, Lamothe A, Corsten M. Lemierre syndrome: presentation of three cases. J Otolaryngol. 2005;34(5):352–358. - PubMed
-
- Vogel M, Horger M. Lemierre syndrome. Article in German. Rofo. 2005;177(1):1–3. - PubMed
-
- Shimada M, Morinaga Y, Kitazaki T, et al. A severe case of Lemierre syndrome with Streptococcus constellatus infection. Jpn J Infect Dis. 2014;67(6):488–489. - PubMed
-
- Benhayoun M, Llor J, Van-Den-Abbeele T, et al. Bilateral jugular thrombosis in Lemierre syndrome. Article in French. Arch Pediatr. 2003;10(12):1071–1074. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
