

Technical Feasibility of Subaxial Cervical Pedicle Screws for Distal Anchoring of Occipitocervical Fixation Constructs in the Mid-Cervical Spine: Early Clinical Experience
- PMID: 35855245
- PMCID: PMC9285641
- DOI: 10.7759/cureus.25964
Technical Feasibility of Subaxial Cervical Pedicle Screws for Distal Anchoring of Occipitocervical Fixation Constructs in the Mid-Cervical Spine: Early Clinical Experience
Abstract
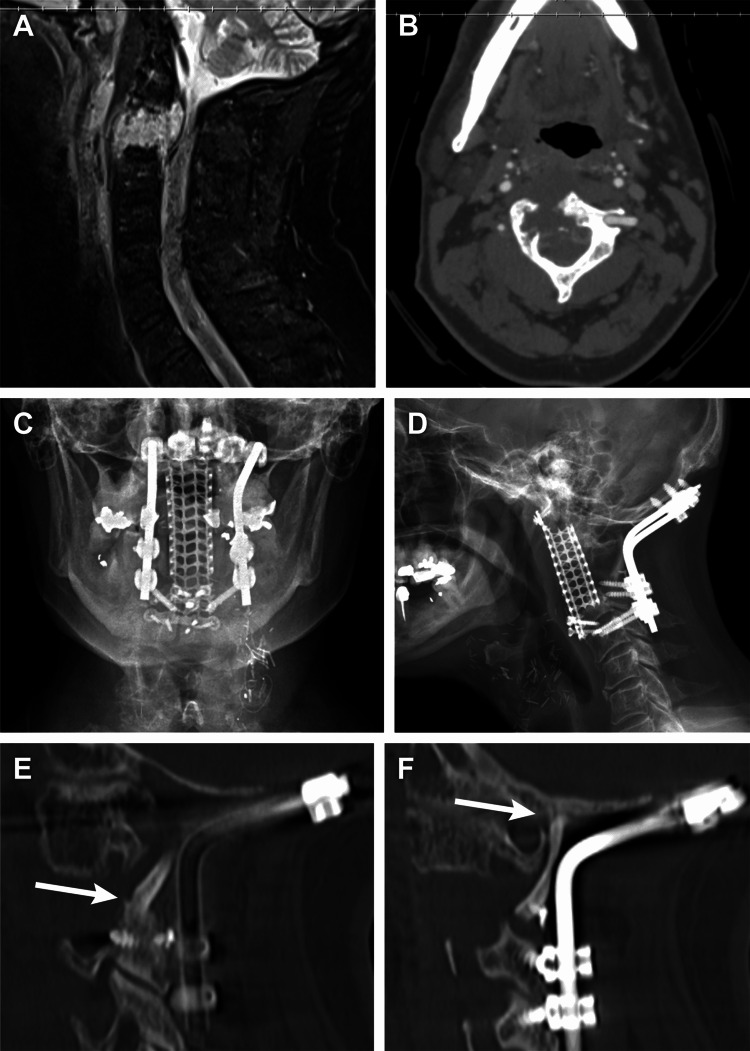
Occipitocervical fixation and fusion (OCF) is performed for patients who have destabilizing traumatic injuries or pathologies affecting the complex bony and ligamentous structures of the occipitoatlantal and atlantoaxial joint structures. Distal fixation failure and pseudoarthrosis are known risks of these constructs, especially for those constructs ending in the mid-cervical spine. We present the technical feasibility of using cervical pedicle screws (CPSs) as distal fixation anchors to strengthen OCF constructs ending in the mid-cervical spine and present a case series describing our early clinical experience with this technique. We used a freehand technique to place subaxial pedicle screws in the mid-cervical spine as the distal fixation point in OCF constructs. This technique involves performing a laminotomy to provide direct visualization of the pedicle borders to safely guide freehand pedicle screw placement. Our early clinical experience with this technique is presented. Three patients received OCF constructs ending in the mid-cervical subaxial spine between C3 and C6. CPSs were placed at the distal vertebra in each construct. Stable instrumentation and arthrodesis were confirmed postoperatively in all patients. This freehand technique uses direct visualization of the pedicle to aid in safe and accurate subaxial pedicle screw placement. CPS placement is clinically feasible and increases the robustness of OCF constructs in appropriately selected patients. Larger case series are needed to further validate the safety and effectiveness of this technique.
Keywords: case series; cervical pedicle screws; freehand technique; occipitocervical fusion; subaxial cervical spine.
Copyright © 2022, Bohl et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures



Similar articles
-
Subaxial Cervical Pedicle Screw Placement With Direct Visualization of Pedicle Borders: 2-Dimensional Operative Video.Oper Neurosurg. 2021 Jun 15;21(1):E54. doi: 10.1093/ons/opab086. Oper Neurosurg. 2021. PMID: 33825891
-
Accuracy of freehand pedicle screws versus lateral mass screws in the subaxial cervical spine.Spine Deform. 2020 Oct;8(5):1049-1058. doi: 10.1007/s43390-020-00119-z. Epub 2020 Apr 20. Spine Deform. 2020. PMID: 32314180
-
The "slide technique"-a novel free-hand method of subaxial cervical pedicle screw placement.BMC Musculoskelet Disord. 2020 Jun 23;21(1):399. doi: 10.1186/s12891-020-03420-0. BMC Musculoskelet Disord. 2020. PMID: 32576178 Free PMC article.
-
Posterior screw fixation in the subaxial cervical spine: a technique and literature review.J Spine Surg. 2020 Mar;6(1):252-261. doi: 10.21037/jss.2019.09.28. J Spine Surg. 2020. PMID: 32309663 Free PMC article. Review.
-
Accuracy and safety assessment of subaxial cervical pedicle screw instrumentation: a systematic review.Spine J. 2025 May 5:S1529-9430(25)00237-2. doi: 10.1016/j.spinee.2025.05.006. Online ahead of print. Spine J. 2025. PMID: 40334991 Review.
References
-
- Occipito-cervical fusion. Indications, technique and results. Hamblen DL. https://pubmed.ncbi.nlm.nih.gov/4960010. J Bone Joint Surg Br. 1967;49:33–45. - PubMed
-
- Total cervicalspine fusion for neck paralysis. Perry J, Nickel VL. https://journals.lww.com/jbjsjournal/Citation/1959/41010/Total_Cervical_.... J Bone Joint Surg Am. 1959;41-A:37–60. - PubMed
-
- Indications and technics for early stabilization of the neck in some fracture dislocations of the cervical spine. RO RA, SO WO. South Med J. 1960;53:565–579. - PubMed
-
- Occipitocervical fusion. Indications, technique, and long-term results in thirteen patients. Wertheim SB, Bohlman HH. https://journals.lww.com/jbjsjournal/Abstract/1987/69060/Occipitocervica.... J Bone Joint Surg Am. 1987;69:833–836. - PubMed
-
- Threaded steinmann pin fusion of the craniovertebral junction. Apostolides PJ, Dickman CA, Golfinos JG, Papadopoulos SM, Sonntag VK. Spine (Phila Pa 1976) 1996;21:1630–1637. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous