

Do neurocognitive impairments explain the differences between brain tumor patients and their proxies when assessing the patient's IADL?
- PMID: 35855454
- PMCID: PMC9290871
- DOI: 10.1093/nop/npac016
Do neurocognitive impairments explain the differences between brain tumor patients and their proxies when assessing the patient's IADL?
Abstract
Background: Neurocognitive impairments are common among brain tumor patients, and may impact patients' awareness of performance in instrumental activities in daily life (IADL). We examined differences between patient- and proxy-reported assessments of the patient's IADL, and whether the level of (dis)agreement is associated with neurocognitive impairments.
Methods: Brain tumor patients and their proxies completed the phase 3 version of the EORTC IADL-BN32 questionnaire measuring IADL, and patients completed six neurocognitive measures. Patient-proxy difference scores in IADL were compared between patients who were defined as neurocognitively impaired (≥2 neurocognitive measures ≥2.0 standard deviations below healthy controls) and non-neurocognitively impaired. With multinomial logistic regression analyses we examined if neurocognitive variables were independently associated with patient-proxy disagreement in IADL ratings.
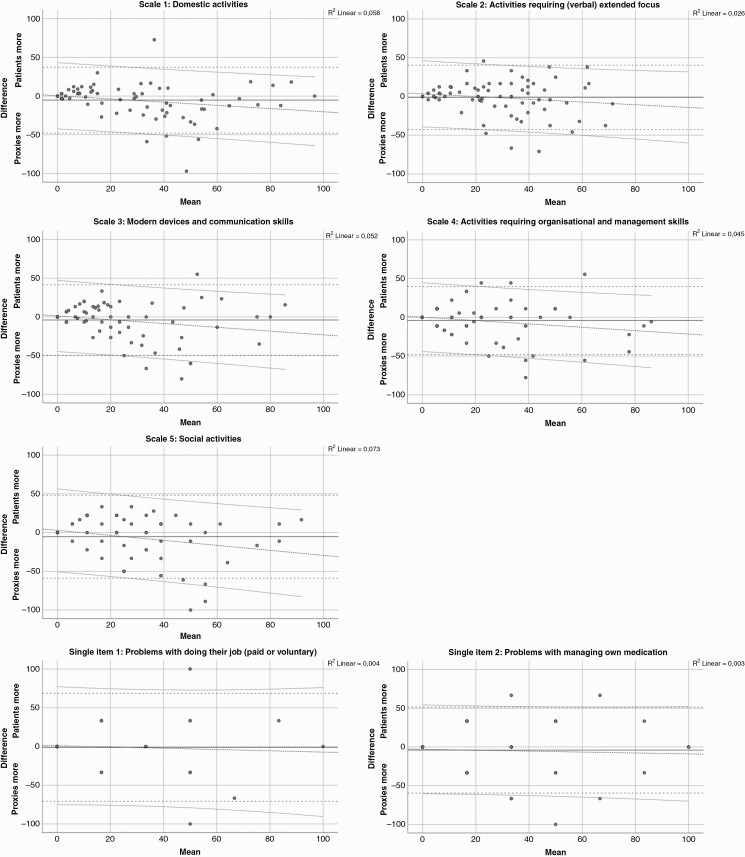
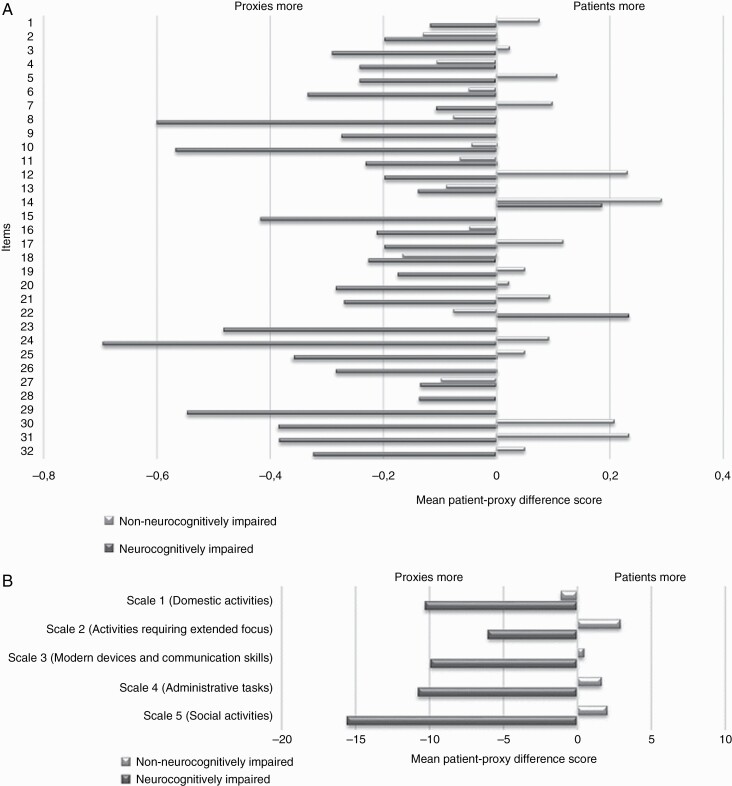
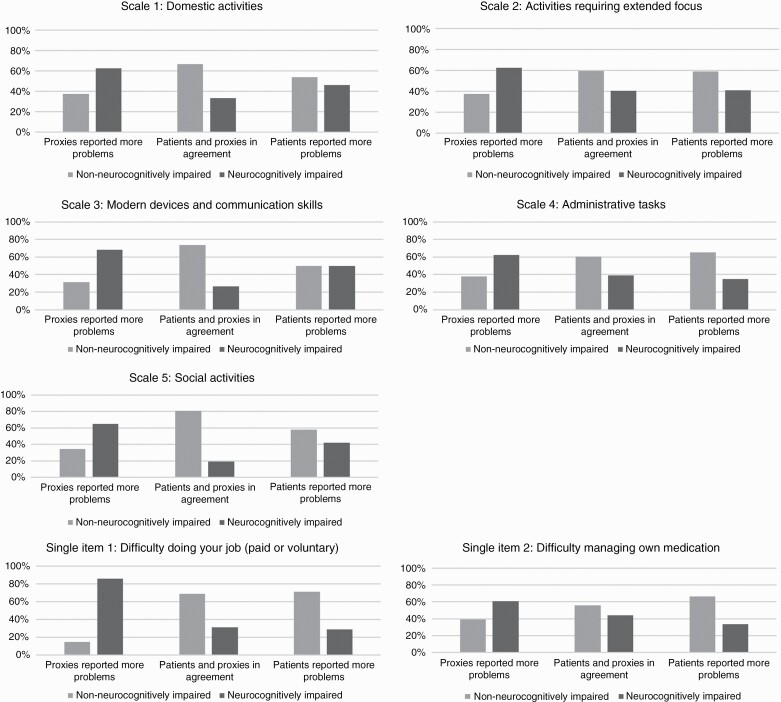
Results: Patients (n = 81) did not systematically (P < .01) rate IADL outcomes different than their proxies. Proxies did report more problems on 19/32 individual items and all five scales. This effect was more apparent in dyads with a neurocognitively impaired patient (n = 37), compared to dyads with non-neurocognitively impaired patients (n = 44). Multinomial logistic regression analyses showed that several neurocognitive variables (e.g., cognitive flexibility and verbal fluency) were independently associated with disagreement between patients and proxies on different scales.
Conclusion: Neurocognitive deficits seem to play a role in the discrepancies between brain tumor patients and their proxies assessment of patient's level of IADL. Although replication of our results is needed, our findings suggests that caution is warranted in interpreting self-reported IADL by patients with neurocognitive impairment, and that such self-reports should be supplemented with proxy ratings.
Keywords: IADL; brain tumor; daily functioning; instrumental activities of daily living; observer-reported; patient-reported.
© The Author(s) 2022. Published by Oxford University Press on behalf of the Society for Neuro-Oncology and the European Association of Neuro-Oncology.
Figures
References
-
- Tucha O, Smely C, Preier M, Lange KW. Cognitive deficits before treatment among patients with brain tumors. Neurosurgery. 2000; 47(2): 324–33-; discussion 33–34. - PubMed
-
- Bartolomei F, Bosma I, Klein M, et al. . How do brain tumors alter functional connectivity? A magnetoencephalography study. Ann Neurol. 2006;59(1):128–138. - PubMed
-
- Derks J, Reijneveld JC, Douw L. Neural network alterations underlie cognitive deficits in brain tumor patients. Curr Opin Oncol. 2014;26(6):627–633. - PubMed
