

Outcomes of Severe Fungal Keratitis Using in vivo Confocal Microscopy and Early Therapeutic Penetrating Keratoplasty
- PMID: 35855739
- PMCID: PMC9288216
- DOI: 10.2147/OPTH.S358709
Outcomes of Severe Fungal Keratitis Using in vivo Confocal Microscopy and Early Therapeutic Penetrating Keratoplasty
Abstract
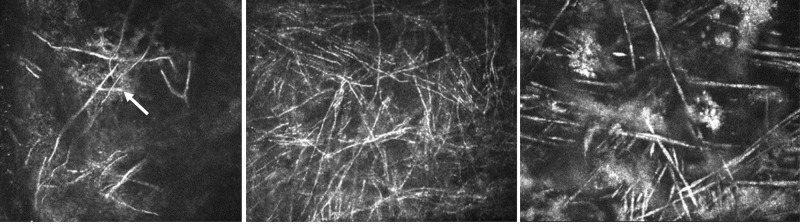
Purpose: The purpose of this study was to assess the impact of early diagnosis using in vivo confocal microscopy and early therapeutic penetrating keratoplasty (TPK) on the outcomes of severe cases of fungal keratitis.
Methods: This retrospective single-center study included 38 patients (40 eyes) with fungal keratitis who presented between December 2013 and February 2020. Preoperative, intraoperative, and postoperative parameters were recorded to assess the role of early correct diagnosis and early surgical therapy on visual acuity outcome and enucleation rate during follow-up.
Results: The mean patient age was 51 years (71% females). The initial external diagnosis was correct in 20 cases (50%). The mean time from symptom onset until admission to our department was 46.8 ± 68.0 (median 28.5) days. The mean time to correct diagnosis after admission to our department was 1 day with in vivo confocal microscopy (IVCM). IVCM was performed in 38 cases, of which 36 (sensitivity: 94.7%) were positive for fungal infection. Twenty-seven out of 40 (67.5%) eyes received a TPK 4.2 ± 3.9 days after admission, with a mean graft size of 8.9 ± 1.9 mm. Three eyes (7.5%) were enucleated. The corrected distance visual acuity of the entire study population increased from 2.0 ± 1.2 LogMAR to 0.96 ± 1.17 LogMAR.
Conclusion: In vivo confocal microscopy is a powerful tool for the early detection of fungal organisms in infectious keratitis. An early TPK with a large graft helps to eradicate the infection timely and results in a favorable visual acuity outcome and lower enucleation rate, especially when treating filamentous fungi.
Keywords: fungal keratitis; in vivo confocal microscopy; penetrating keratoplasty.
© 2022 Sourlis et al.
Figures




Similar articles
-
Outcomes of therapeutic deep lamellar keratoplasty and penetrating keratoplasty for advanced infectious keratitis: a comparative study.Ophthalmology. 2009 Apr;116(4):615-23. doi: 10.1016/j.ophtha.2008.12.043. Epub 2009 Feb 25. Ophthalmology. 2009. PMID: 19243833
-
Excisional penetrating keratoplasty for fungal interface keratitis after endothelial keratoplasty: surgical timing and visual outcome.Int Ophthalmol. 2021 Jan;41(1):363-373. doi: 10.1007/s10792-020-01576-1. Epub 2020 Sep 17. Int Ophthalmol. 2021. PMID: 32940829 Review.
-
Outcomes of therapeutic penetrating keratoplasty in 198 eyes with fungal keratitis.Indian J Ophthalmol. 2019 Oct;67(10):1599-1605. doi: 10.4103/ijo.IJO_1952_18. Indian J Ophthalmol. 2019. PMID: 31546488 Free PMC article.
-
Recurrence of Infection in Corneal Grafts After Therapeutic Penetrating Keratoplasty for Microbial Keratitis.Cornea. 2020 Jan;39(1):39-44. doi: 10.1097/ICO.0000000000002044. Cornea. 2020. PMID: 31259861
-
Infectious interface keratitis (IIK) following lamellar keratoplasty: A literature review.Ocul Surf. 2019 Oct;17(4):635-643. doi: 10.1016/j.jtos.2019.08.001. Epub 2019 Aug 12. Ocul Surf. 2019. PMID: 31415815
Cited by
-
Efficacy of the Combined Intrastromal Injection of Voriconazole and Amphotericin B in Recalcitrant Fungal Keratitis.Microorganisms. 2024 Apr 30;12(5):922. doi: 10.3390/microorganisms12050922. Microorganisms. 2024. PMID: 38792749 Free PMC article.
-
Trans-kingdom fungal pathogens infecting both plants and humans, and the problem of azole fungicide resistance.Front Microbiol. 2024 Feb 12;15:1354757. doi: 10.3389/fmicb.2024.1354757. eCollection 2024. Front Microbiol. 2024. PMID: 38410389 Free PMC article. Review.
-
[Fungal keratitis in Germany : Diagnostics, conservative and microsurgical treatment].Ophthalmologie. 2025 Aug;122(8):652-669. doi: 10.1007/s00347-025-02274-y. Epub 2025 Jul 24. Ophthalmologie. 2025. PMID: 40705069 Review. German.
-
[Bacterial keratitis : Clinical aspects, pathogens and treatment].Ophthalmologie. 2024 Sep;121(9):769-782. doi: 10.1007/s00347-024-02102-9. Epub 2024 Aug 20. Ophthalmologie. 2024. PMID: 39162822 Review. German.
-
[Bilateral chronic contact lens-associated keratitis].Ophthalmologie. 2024 May;121(5):410-414. doi: 10.1007/s00347-024-01993-y. Epub 2024 Feb 5. Ophthalmologie. 2024. PMID: 38315191 German. No abstract available.
References
LinkOut - more resources
Full Text Sources
