

Tumor-Induced Osteomalacia: A Systematic Clinical Review of 895 Cases
- PMID: 35857061
- PMCID: PMC9474374
- DOI: 10.1007/s00223-022-01005-8
Tumor-Induced Osteomalacia: A Systematic Clinical Review of 895 Cases
Abstract
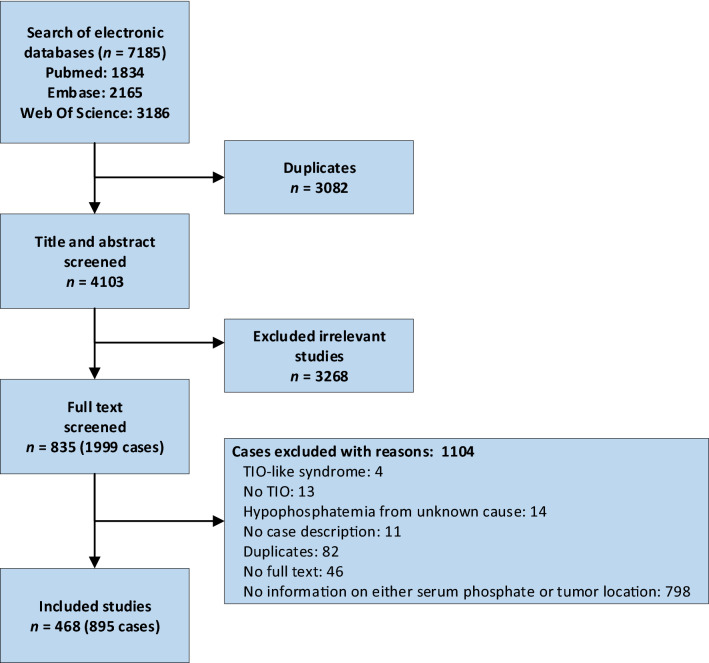
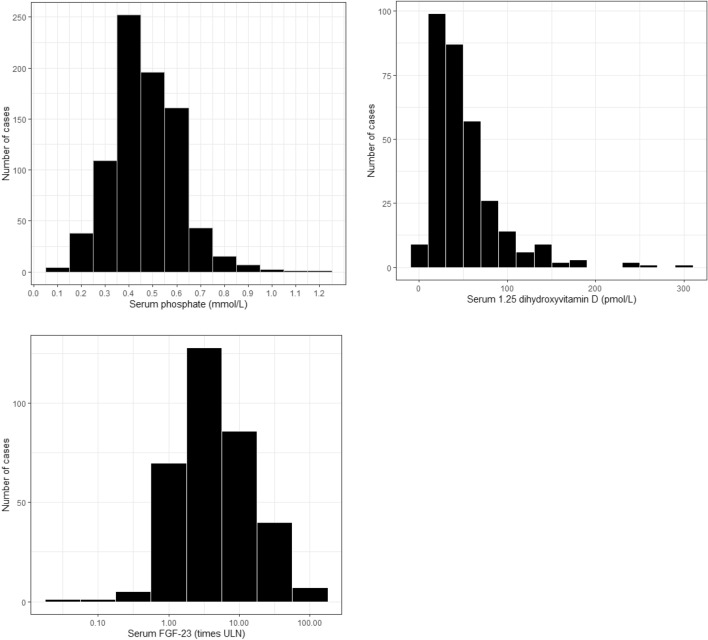
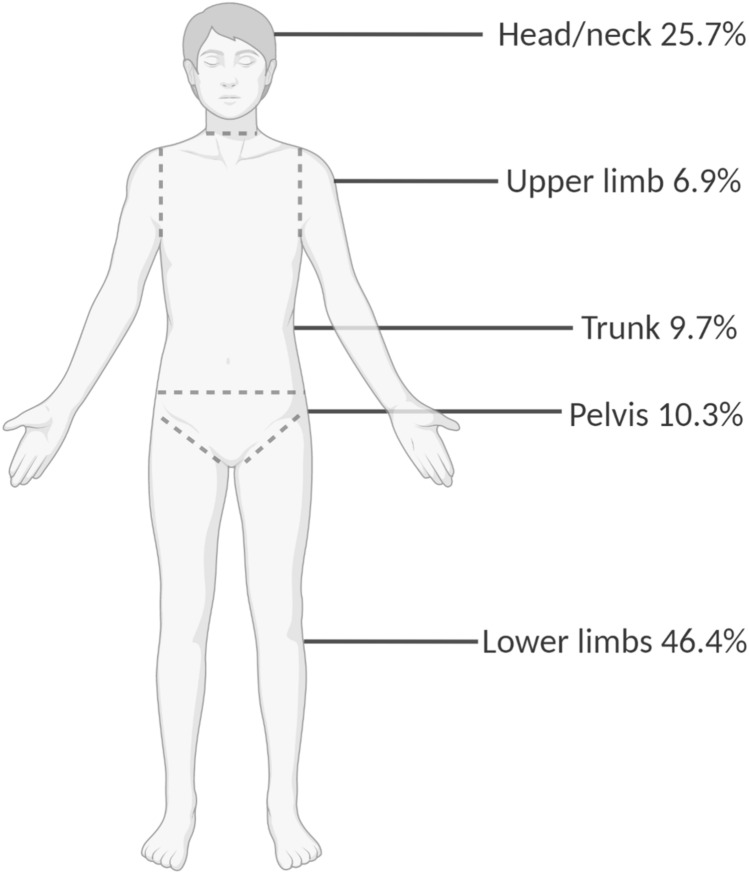
Tumor-induced osteomalacia (TIO) is a rare and largely underdiagnosed paraneoplastic condition. Previous reviews often reported incomplete data on clinical aspects, diagnosis or prognosis. The aim of this study was to present a systematic clinical review of all published cases of TIO. A search was conducted in Pubmed, Embase, Web of Science from inception until April 23rd, 2020. We selected case reports and case series of patients diagnosed with TIO, with information on tumor localization and serum phosphate concentration. Two reviewers independently extracted data on biochemical and clinical characteristics including bone involvement, tumor localization and treatment. 468 articles with 895 unique TIO cases were included. Median age was 46 years (range 9 months-90 years) and 58.3% were males. Hypophosphatemia and inappropriately low or normal 1,25-dihydroxyvitamin D levels, characteristic for TIO, were present in 98% of cases. Median tumor size was 2.7 cm (range 0.5 to 25.0 cm). Serum fibroblast growth factor 23 was related to tumor size (r = 0.344, P < 0.001). In 32% of the cases the tumor was detected by physical examination. Data on bone phenotype confirmed skeletal involvement: 62% of cases with BMD data had a T-score of the lumbar spine ≤ - 2.5 (n = 61/99) and a fracture was reported in at least 39% of all cases (n = 346/895). Diagnostic delay was longer than 2 years in more than 80% of cases. 10% were reported to be malignant at histology. In conclusion, TIO is a debilitating disease characterized by a long diagnostic delay leading to metabolic disturbances and skeletal impairment. Increasing awareness of TIO should decrease its diagnostic delay and the clinical consequences.
Keywords: FGF23; Fracture; Hypophosphatemia; Osteomalacia; Rickets; Tumor-induced osteomalacia.
© 2022. The Author(s).
Conflict of interest statement
AB is supported by a Grant from Health ~ Holland (PhosphoNorm; LSHM18029). AP, JV WX, and JB declare they have no financial interests. SB received grants from Ultragenyx and consulting fees from Ultragenyx, Amgen and Inozyme. SB serves on the Data Safety Monitory Board of NIDCR (NIH) and NIDDK (FIT4KIDS); on the advisory board of Ultragenyx, Amgen and Inozyme; and in the scientific advisory board of the XLH network. SF received lecture fees from Kyowa Kirin, and is president of the Japanese Society for Bone and Mineral Research (JSBMR). SM served as speaker for Abiogen, Bruno Farmaceutici, Diasorin, Kyowa Kirin, UCB. He also served in advisory boards of Eli Lilly, Kyowa Kirin, UCB. MCZ reports that her institution has received a research grant from Kyowa Kirin and she is an unpaid board member of the steering committee of the Kyowa Kirin International XLH registry.
Figures
References
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Miscellaneous
