

Efficacy and Safety of Add-on Mirogabalin to NSAIDs in Lumbar Spinal Stenosis with Peripheral Neuropathic Pain: A Randomized, Open-Label Study
- PMID: 35857196
- PMCID: PMC9298169
- DOI: 10.1007/s40122-022-00410-z
Efficacy and Safety of Add-on Mirogabalin to NSAIDs in Lumbar Spinal Stenosis with Peripheral Neuropathic Pain: A Randomized, Open-Label Study
Erratum in
-
Correction to: Efficacy and Safety of Add-on Mirogabalin to NSAIDs in Lumbar Spinal Stenosis with Peripheral Neuropathic Pain: A Randomized, Open-Label Study.Pain Ther. 2022 Dec;11(4):1215-1217. doi: 10.1007/s40122-022-00441-6. Pain Ther. 2022. PMID: 36203079 Free PMC article. No abstract available.
Abstract
Introduction: In Japan, conservative therapy for patients with lumbar spinal stenosis (LSS) includes non-steroidal anti-inflammatory drugs (NSAIDs), prostaglandin E1, tramadol, physical/exercise therapy, and nerve blocks. Mirogabalin, a selective oral α2δ ligand, is approved for treating peripheral neuropathic pain, though data regarding visual analog scores (VAS) for pain in patients with LSS are limited. We investigated the efficacy and safety of mirogabalin as an add-on treatment in patients with LSS taking NSAIDs compared with patients taking NSAIDs only.
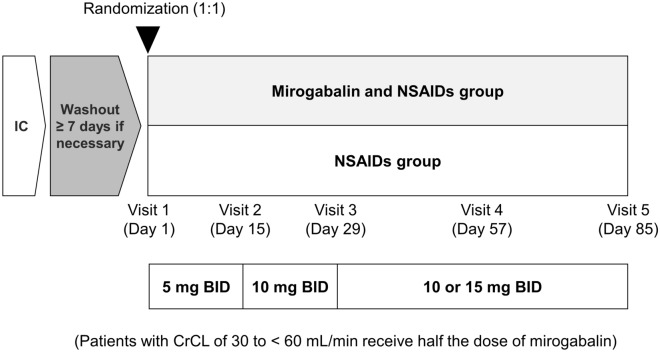
Methods: This multicenter, randomized, open-label study (MiroTAS) was conducted at 32 centers in Japan between June 2020 and October 2021. Patients were randomly assigned to mirogabalin and NSAIDs or NSAIDs alone in a 1:1 ratio. NSAIDs were administered according to their Japanese package inserts; mirogabalin was administered based on renal function [creatinine clearance (CrCL) ≥ 60 mL/min, 5 mg twice daily (BID) in Weeks 1-2, 10 mg BID in Weeks 3-4, and 15 or 10 mg BID after Week 5; CrCL 30 to < 60 mL/min, 2.5 mg BID Weeks 1-2, 5 mg BID Weeks 3-4, and 7.5 or 5 mg BID after Week 5]. The primary endpoint was the change in VAS score for leg pain from baseline to Week 12. Secondary endpoints were quality of life, evaluated using the EuroQol five-dimensional descriptive system (EQ-5D-5L) (at baseline and Week 12) and Patient Global Impression of Change (PGIC) (at Week 12), and safety. Change in VAS score at Week 12 was calculated using a linear mixed model for repeated measures. The safety endpoints were treatment-emergent adverse events (TEAEs) and adverse drug reactions.
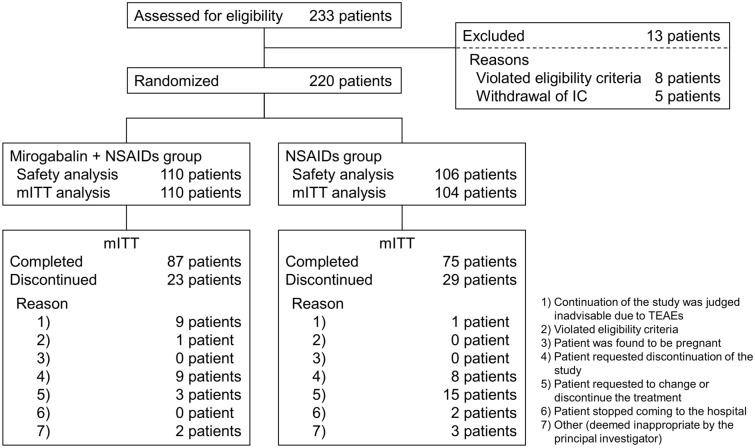
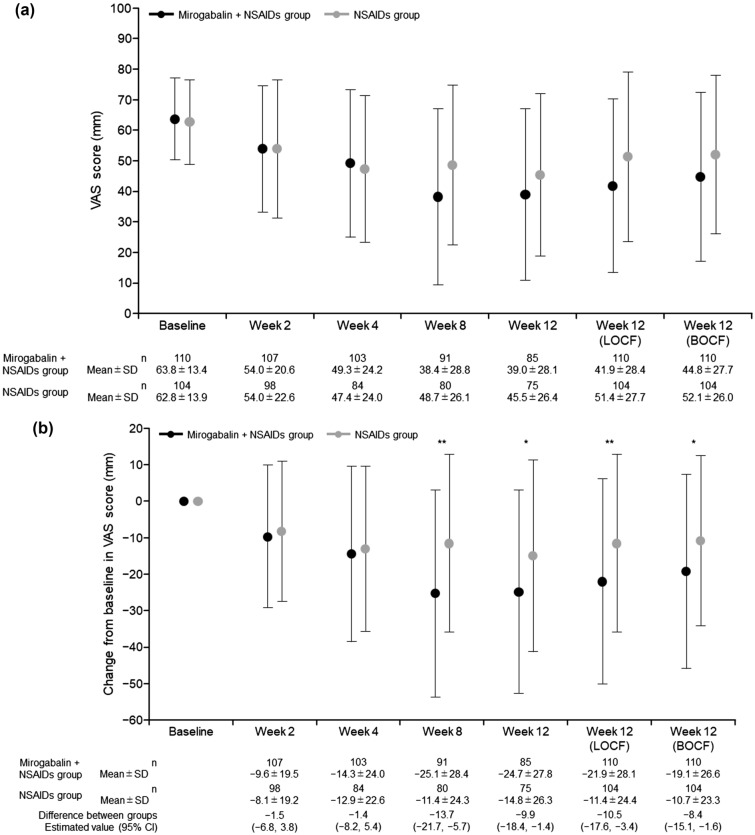
Results: In total, 220 patients who met the eligibility criteria were enrolled. In the mirogabalin and NSAIDs and NSAIDs groups, mean ages (67.8 vs. 70.9 years), proportions of female patients (54.5% vs. 49.0%), mean body weights (63.9 vs. 62.0 kg), mean CrCL values (81.5 vs. 70.7 mL/min), proportions of patients with CrCL 30 to < 60 mL/min (27.3% vs. 33.7%), mean VAS scores (63.8 vs. 62.8 mm), and proportions of patients with VAS score ≥ 60 (53.6% vs. 52.9%) at enrollment were similar. The median durations of LSS were 9.0 and 11.0 months and the spine pain DETECT questionnaire (SPDQ) scores were 6.8 and 7.8, respectively. The least square (LS) mean change in VAS score from baseline to Week 12 was - 24.1 mm in the mirogabalin and NSAIDs group and - 14.2 mm in the NSAIDs group (both P < 0.0001 vs. baseline). The difference in LS mean was - 9.9 [95% confidence interval (CI), - 18.0, - 1.8] (P = 0.0174). The improvement in EQ-5D-5L score at Week 12 was significantly greater in the mirogabalin and NSAIDs group versus the NSAIDs group [mean difference, 0.0529 (95% CI, 0.0036, 0.1022), P = 0.0357]. At Week 12, the proportions of patients with PGIC scores ≤ 3 and ≤ 2 were higher in the mirogabalin and NSAIDs group vs. the NSAIDs group (76.2% vs. 50.0%, P = 0.0006, and 47.6% vs. 32.4%, P = 0.0523). In the mirogabalin and NSAIDs group, the incidences of TEAEs and adverse drug reactions were 60.9% and 57.3%, respectively, and the most common TEAEs were somnolence (30.0%) and dizziness (25.5%).
Conclusions: The addition of mirogabalin to NSAIDs improved VAS, EQ-5D-5L, and PGIC. The main TEAEs were somnolence and dizziness. The addition of mirogabalin to NSAIDs improved peripheral neuropathic pain associated with LSS and raised no new safety concerns.
Trial registration: Japan Registry of Clinical Trials (jRCTs021200007).
Keywords: Lumbar spinal stenosis; Mirogabalin; NSAIDs; Peripheral neuropathic pain; α2δ ligands.
© 2022. The Author(s).
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous
