

Understanding the multidimensional cognitive deficits of logopenic variant primary progressive aphasia
- PMID: 35857482
- PMCID: PMC9473356
- DOI: 10.1093/brain/awac208
Understanding the multidimensional cognitive deficits of logopenic variant primary progressive aphasia
Abstract
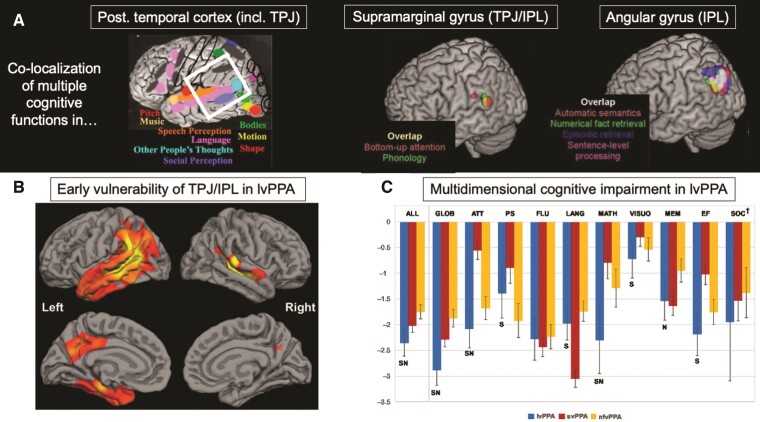
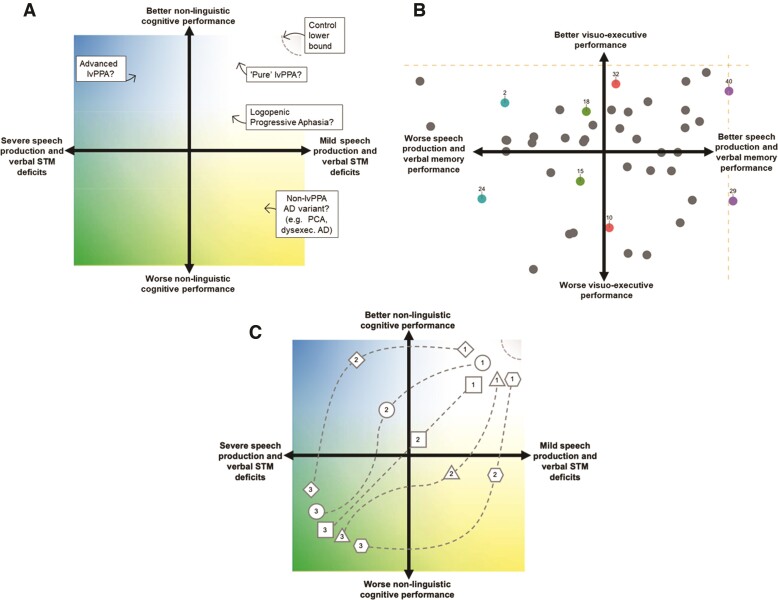
The logopenic variant of primary progressive aphasia is characterized by early deficits in language production and phonological short-term memory, attributed to left-lateralized temporoparietal, inferior parietal and posterior temporal neurodegeneration. Despite patients primarily complaining of language difficulties, emerging evidence points to performance deficits in non-linguistic domains. Temporoparietal cortex, and functional brain networks anchored to this region, are implicated as putative neural substrates of non-linguistic cognitive deficits in logopenic variant primary progressive aphasia, suggesting that degeneration of a shared set of brain regions may result in co-occurring linguistic and non-linguistic dysfunction early in the disease course. Here, we provide a Review aimed at broadening the understanding of logopenic variant primary progressive aphasia beyond the lens of an exclusive language disorder. By considering behavioural and neuroimaging research on non-linguistic dysfunction in logopenic variant primary progressive aphasia, we propose that a significant portion of multidimensional cognitive features can be explained by degeneration of temporal/inferior parietal cortices and connected regions. Drawing on insights from normative cognitive neuroscience, we propose that these regions underpin a combination of domain-general and domain-selective cognitive processes, whose disruption results in multifaceted cognitive deficits including aphasia. This account explains the common emergence of linguistic and non-linguistic cognitive difficulties in logopenic variant primary progressive aphasia, and predicts phenotypic diversification associated with progression of pathology in posterior neocortex.
Keywords: Alzheimer’s disease; inferior parietal lobe; language; non-linguistic functions; primary progressive aphasia; temporoparietal junction.
© The Author(s) 2022. Published by Oxford University Press on behalf of the Guarantors of Brain.
Figures
References
-
- Mesulam MM. Primary progressive aphasia. Ann Neurol. 2001;49:425–432. - PubMed
-
- Mesulam MM. Slowly progressive aphasia without generalized dementia. Ann Neurol. 1982;11:592–598. - PubMed
-
- Weintraub S, Rubin NP, Mesulam MM. Primary progressive aphasia. Longitudinal course, neuropsychological profile, and language features. Arch Neurol. 1990;47:1329–1335. - PubMed
