

Obstetrical Outcomes After Implementation of Laborist Model During the COVID-19 Pandemic
- PMID: 35858475
- PMCID: PMC9696682
- DOI: 10.1097/PTS.0000000000001066
Obstetrical Outcomes After Implementation of Laborist Model During the COVID-19 Pandemic
Abstract
Objective: The COVID-19 pandemic prompted labor and delivery units to establish ways to decrease viral exposure to healthcare workers while continuing to deliver optimal patient care. A laborist model was implemented to improve safety at our tertiary care hospital in Long Island. The aim of the study is to determine whether implementation of a laborist model during the COVID-19 pandemic is associated with a change in the frequency of cesarean birth.
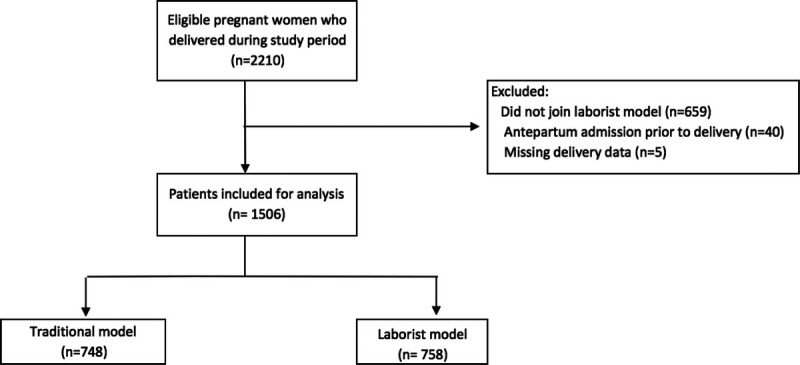
Methods: The retrospective cohort study included patients who delivered at a single tertiary center during March 2019 to May 2019 and March 2020 to May 2020 when our laborist model was initiated. The primary outcome compared the frequency of a cesarean delivery between both models. Secondary outcomes were the frequency of adverse obstetrical complications, which included intensive care unit admission, shoulder dystocia, intra-amniotic infection, hemorrhage, and need for blood transfusion. Statistical analysis included multivariable regression to adjust for potential confounders.
Results: A total of 1506 patients were included. Baseline characteristics were similar between the 2 groups. After adjusting for potential confounders, there was no significant difference in the frequency of cesarean births between both models (37% versus 35%; adjusted odds ratio, 1.003; 95% confidence interval, 0.46-2.89). Similarly, there were no significant differences in adverse outcomes between the study populations (adjusted odds ratio, 1.064; 95% confidence interval, 0.68-1.59).
Conclusions: A change in practice behavior during a pandemic was not associated with an increase in frequency of cesarean births or adverse obstetrical outcomes.
Copyright © 2022 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
The authors disclose no conflict of interest.
References
-
- Centers for Disease Control and Prevention . Coronavirus disease 2019 (COVID-19). Considerations for Inpatient Obstetric Healthcare Settings. 2020. Available at: https://www.cdc.gov/coronavirus/2019-ncov/hcp/inpatient-obstetric-health.... Accessed July 16, 2020.
-
- Caron C, Van Syckle K. Some pregnant women in New York City will have to delivery babies alone. New York Times. 2020;13.
-
- Srinivas SK, Small DS, Macheras M. Evaluating the impact of the laborist model of obstetric care on maternal and neonatal outcomes. Am J Obstet Gynecol. 2016;215:770.e1–770.e9. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
