

Burden of SARS-CoV-2 infection in healthcare workers during second wave in England and impact of vaccines: prospective multicentre cohort study (SIREN) and mathematical model
- PMID: 35858689
- PMCID: PMC9295077
- DOI: 10.1136/bmj-2022-070379
Burden of SARS-CoV-2 infection in healthcare workers during second wave in England and impact of vaccines: prospective multicentre cohort study (SIREN) and mathematical model
Abstract
Objective: To describe the incidence of, risk factors for, and impact of vaccines on primary SARS-CoV-2 infection during the second wave of the covid-19 pandemic in susceptible hospital healthcare workers in England.
Design: Multicentre prospective cohort study.
Setting: National Health Service secondary care health organisations (trusts) in England between 1 September 2020 and 30 April 2021.
Participants: Clinical, support, and administrative staff enrolled in the SARS-CoV-2 Immunity and Reinfection Evaluation (SIREN) study with no evidence of previous infection. Vaccination status was obtained from national covid-19 vaccination registries and self-reported.
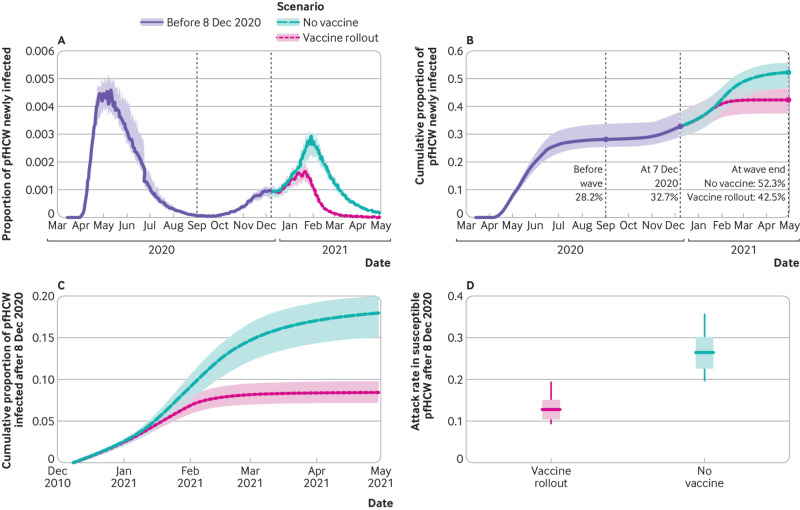
Main outcome measure: SARS-CoV-2 infection confirmed by polymerase chain reaction. Mixed effects logistic regression was conducted to determine demographic and occupational risk factors for infection, and an individual based mathematical model was used to predict how large the burden could have been if vaccines had not been available from 8 December 2020 .
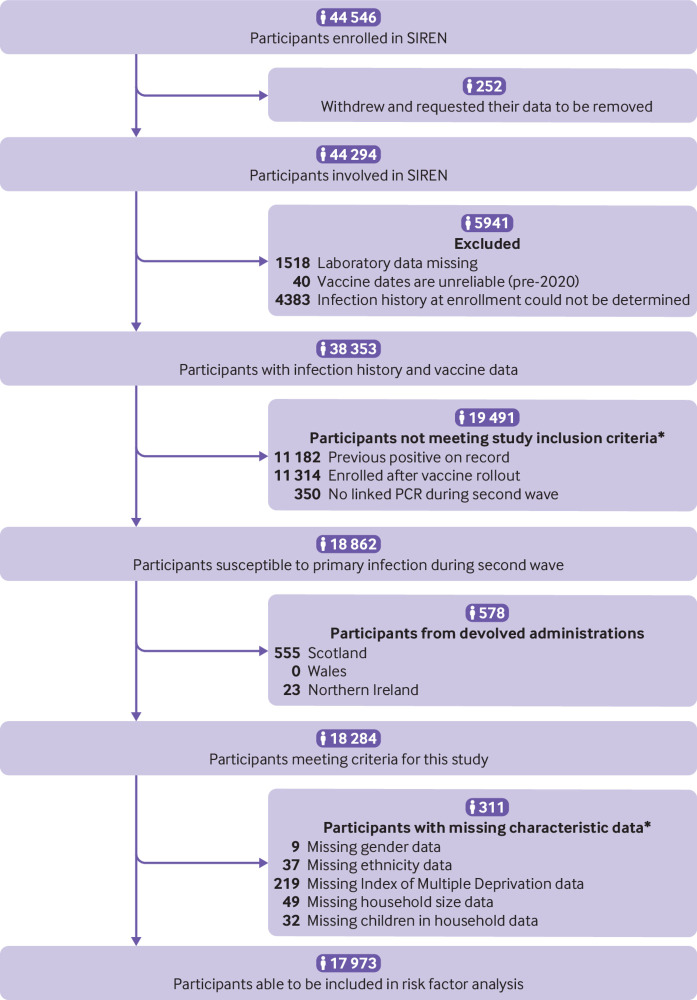
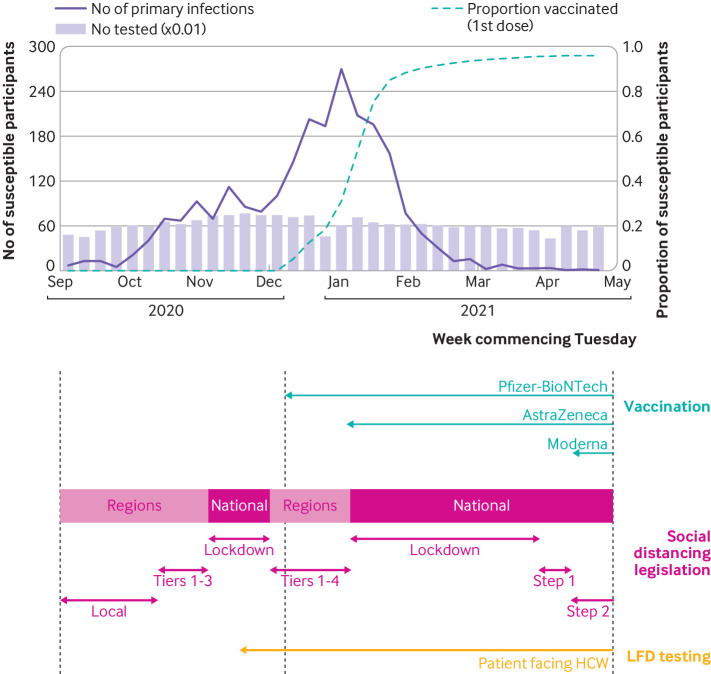
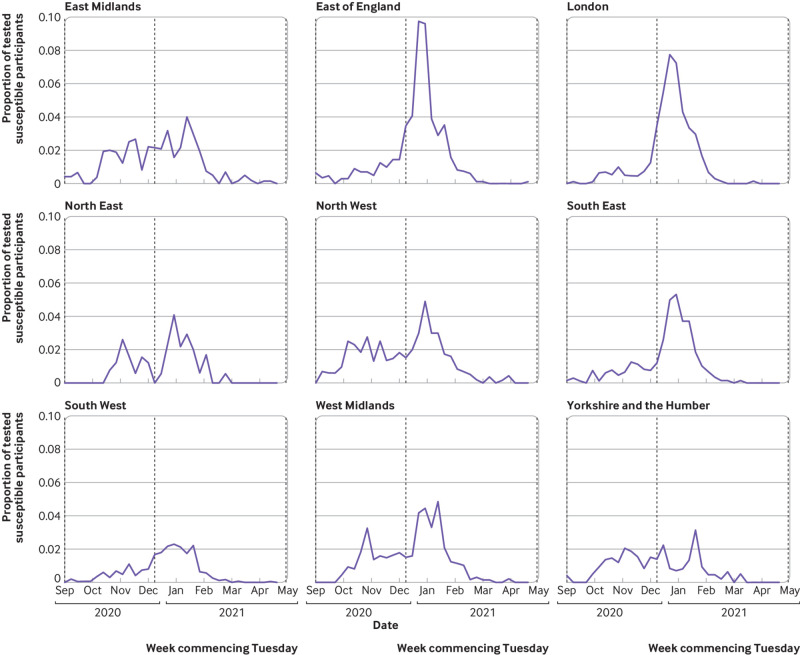
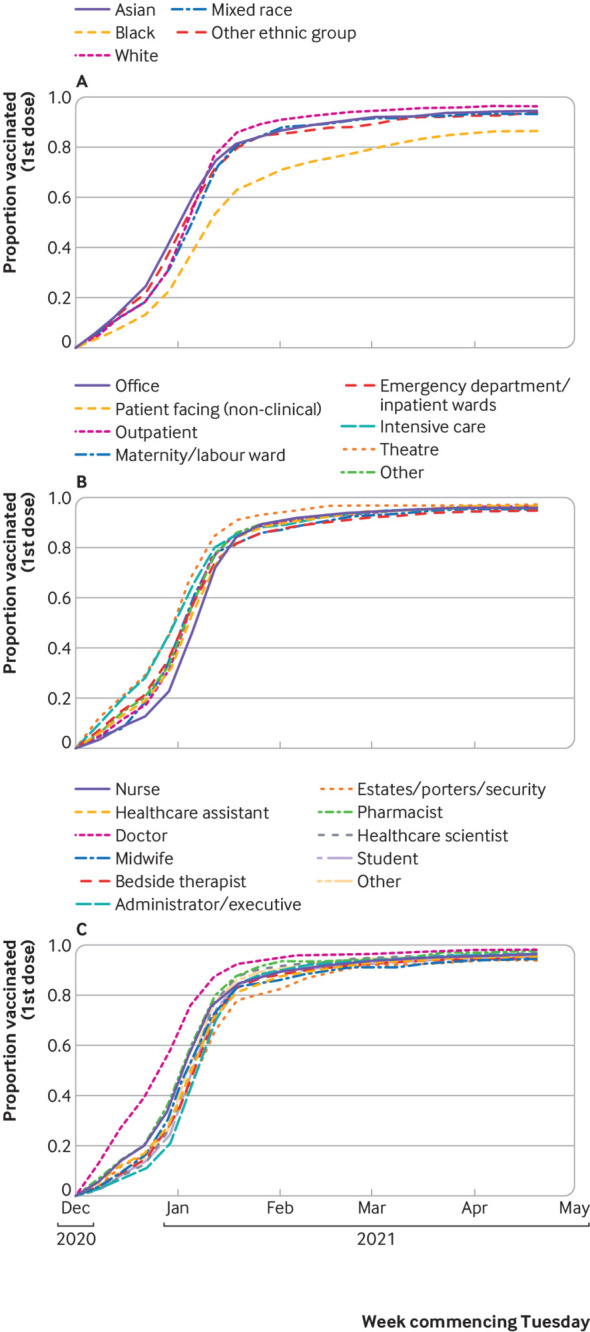
Results: During England's second wave, 12.9% (2353/18 284) of susceptible SIREN participants became infected with SARS-CoV-2. Infections peaked in late December 2020 and decreased from January 2021, concurrent with the cohort's rapid vaccination coverage and a national lockdown. In multivariable analysis, factors increasing the likelihood of infection in the second wave were being under 25 years old (20.3% (132/651); adjusted odds ratio 1.35, 95% confidence interval 1.07 to 1.69), living in a large household (15.8% (282/1781); 1.54, 1.23 to 1.94, for participants from households of five or more people), having frequent exposure to patients with covid-19 (19.2% (723/3762); 1.79, 1.56 to 2.06, for participants with exposure every shift), working in an emergency department or inpatient ward setting (20.8% (386/1855); 1.76, 1.45 to 2.14), and being a healthcare assistant (18.1% (267/1479); 1.43, 1.16 to 1.77). Time to first vaccination emerged as being strongly associated with infection (P<0.001), with each additional day multiplying a participant's adjusted odds ratio by 1.02. Mathematical model simulations indicated that an additional 9.9% of all patient facing hospital healthcare workers would have been infected were it not for the rapid vaccination coverage.
Conclusions: The rapid covid-19 vaccine rollout from December 2020 averted infection in a large proportion of hospital healthcare workers in England: without vaccines, second wave infections could have been 69% higher. With booster vaccinations being needed for adequate protection from the omicron variant, and perhaps the need for further boosters for future variants, ensuring equitable delivery to healthcare workers is essential. The findings also highlight occupational risk factors that persisted in healthcare workers despite vaccine rollout; a greater understanding of the transmission dynamics responsible for these is needed to help to optimise the infection prevention and control policies that protect healthcare workers from infection and therefore to support staffing levels and maintain healthcare provision.
Trial registration: ISRCTN registry ISRCTN11041050.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at https://www.icmje.org/disclosure-of-interest/ and declare: support from the Department of Health and Social Care, UK Health Security Agency, and National Institute for Health Research; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships of activities that could appear to have influenced the submitted work.
Figures
References
-
- UK Health Security Agency. Coronavirus in the UK: Cases in the UK. https://coronavirus.data.gov.uk/details/cases.
-
- Office for National Statistics. Coronavirus (COVID-19) Infection Survey: England. https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/....
-
- Public Health England. PHE investigating a novel variant of COVID-19. 2020. https://www.gov.uk/government/news/phe-investigating-a-novel-variant-of-....
-
- Medicines and Healthcare products Regulatory Agency. UK medicines regulator gives approval for first UK COVID-19 vaccine. 2020. https://www.gov.uk/government/news/uk-medicines-regulator-gives-approval....
Publication types
MeSH terms
Substances
Supplementary concepts
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous