

Outcomes of Biceps Tenotomy Versus Tenodesis During Arthroscopic Rotator Cuff Repair: An Analysis of Patients From a Large Multicenter Database
- PMID: 35859647
- PMCID: PMC9290127
- DOI: 10.1177/23259671221110851
Outcomes of Biceps Tenotomy Versus Tenodesis During Arthroscopic Rotator Cuff Repair: An Analysis of Patients From a Large Multicenter Database
Abstract
Background: Studies to date evaluating biceps tenotomy versus tenodesis in the setting of concomitant rotator cuff repair (RCR) have demonstrated relatively equivalent pain and functional outcomes.
Hypothesis: It was hypothesized that a significant difference could be demonstrated for pain and functional outcome scores comparing biceps tenotomy versus tenodesis in the setting of RCR if the study was adequately powered.
Study design: Cohort study; Level of evidence, 3.
Methods: The Arthrex Surgical Outcomes System database was queried for patients who underwent arthroscopic biceps tenotomy or tenodesis and concomitant RCR between 2013 and 2021; included patients had a minimum of 2 years of follow-up. Outcomes between treatment types were assessed using the American Shoulder and Elbow Surgeons Shoulder (ASES), Single Assessment Numeric Evaluation (SANE), visual analog scale (VAS) for pain, and Veterans RAND 12-Item Health Survey (VR-12) scores preoperatively and at 3 months, 6 months, 1 year, and 2 years postoperatively. Results were stratified by age at surgery (3 groups: <55, 55-65, >65 years) and sex.
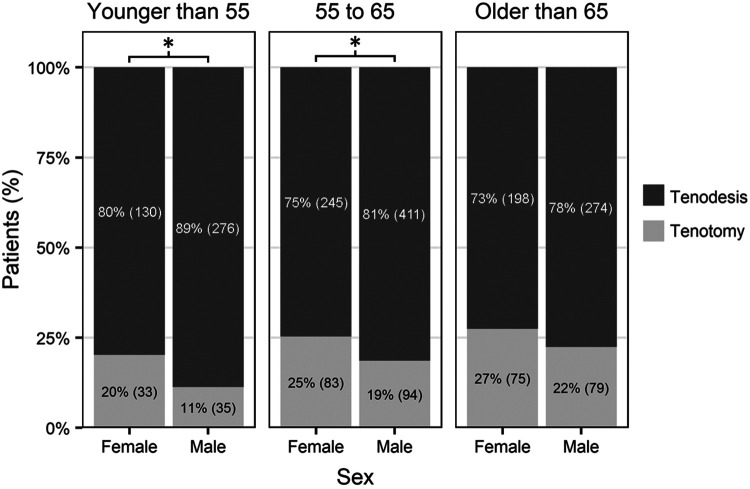
Results: Overall, 1936 primary RCRs were included for analysis (1537 biceps tenodesis and 399 biceps tenotomy patients). Patients who underwent tenotomy were older and more likely to be female. A greater proportion of female patients aged <55 years and 55 to 65 years received a biceps tenotomy compared with tenodesis (P = .012 and .026, respectively). All scores were comparable between the treatment types preoperatively and at 3 months, 6 months, and 1 year postoperatively. At 2-year follow-up, patients who received a biceps tenodesis had statistically more favorable ASES, SANE, VAS pain, and VR-12 scores (P ≤ .031); however, the differences did not exceed the minimal clinically important difference (MCID) for these measures.
Conclusion: Our findings indicate that surgeons are more likely to perform a biceps tenotomy in female and older patients. Biceps tenodesis provided improved pain and functional scores compared with tenotomy at 2-year follow-up; however, the benefit did not exceed previously reported MCID for the outcome scores. Both procedures provided improvement in outcomes; thus, the choice of procedure should be a shared decision between the surgeon and patient.
Keywords: biceps tenodesis; biceps tenotomy; rotator cuff repair.
© The Author(s) 2022.
Conflict of interest statement
One or more of the authors has declared the following potential conflict of interest or source of funding: R.C.S. has received education payments from MedInc, speaking fees from Acumed, and hospitality payments from Integra LifeSciences. T.W.W. has received consulting fees and royalties from Exactech. K.W.F. has received education payments from Exactech; consulting fees from Arthrex, Exactech, and Flexion Therapeutics; speaking fees from Arthrex, Arthrosurface, and CGG Medical; honoraria from Arthrosurface and Baudax Bio; and hospitality payments from Rotation Medical. J.O.W. has received education payments from Pinnacle and hospitality payments from Acumed and Zimmer Biomet. R.P.R. has received grant support from Arthrex and education payments from Arthrex and Smith & Nephew. M.W.M. has received education payments from Fortis Surgical and speaking fees from Arthrex. M.C.F. has received hospitality payments from Arthrex. J.J.K. has received consulting fees from Exactech and hospitality payments from Integra LifeSciences. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Figures
References
-
- Belay ES, Wittstein JR, Garrigues GE, et al. Biceps tenotomy has earlier pain relief compared to biceps tenodesis: a randomized prospective study. Knee Surg Sports Traumatol Arthrosc. 2019;27(12):4032–4037. doi:10.1007/s00167-019-05682 -1 - PubMed
-
- Belk JW, Kraeutler MJ, Houck DA, Chrisman AN, Scillia AJ, McCarty EC. Biceps tenodesis versus tenotomy: a systematic review and meta-analysis of level I randomized controlled trials. J Shoulder Elbow Surg. 2021;30(5):951–960. doi:10.1016/j.jse.2020.11.012 - PubMed
LinkOut - more resources
Full Text Sources
