

Varying Clinical Phenotypes of Mitochondrial DNA T12811C Mutation: A Case Series Report
- PMID: 35860740
- PMCID: PMC9291510
- DOI: 10.3389/fmed.2022.912103
Varying Clinical Phenotypes of Mitochondrial DNA T12811C Mutation: A Case Series Report
Abstract
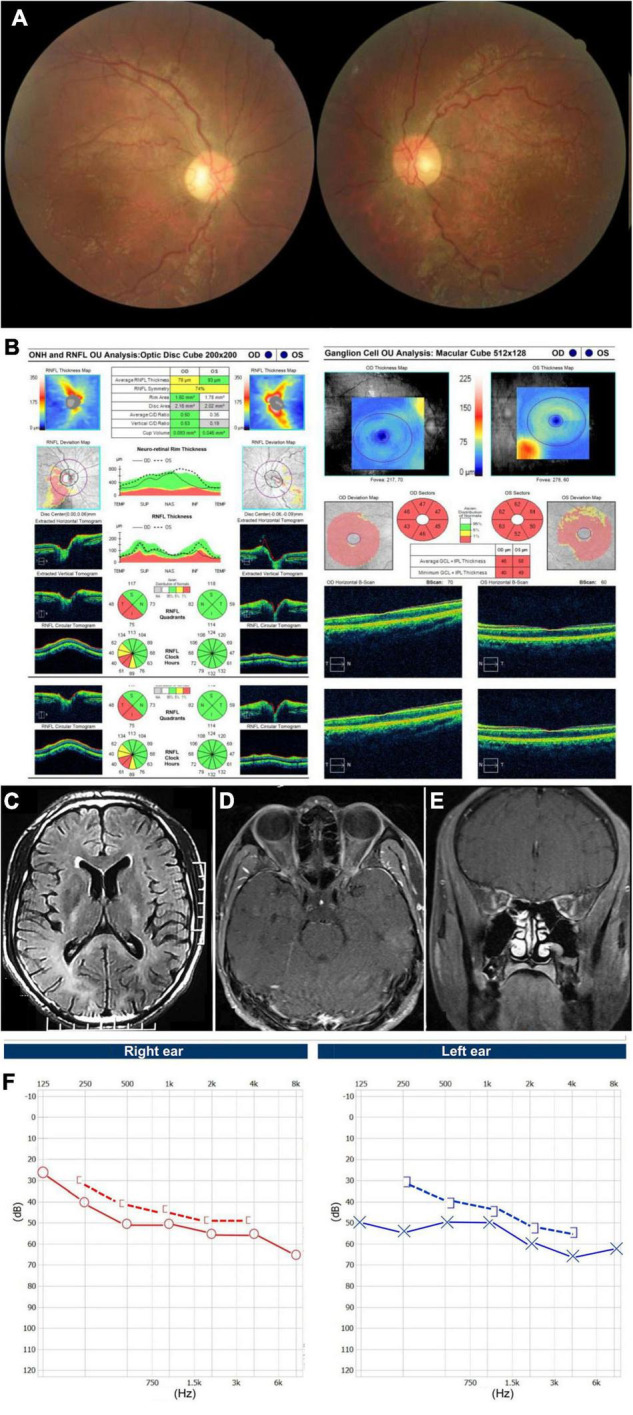
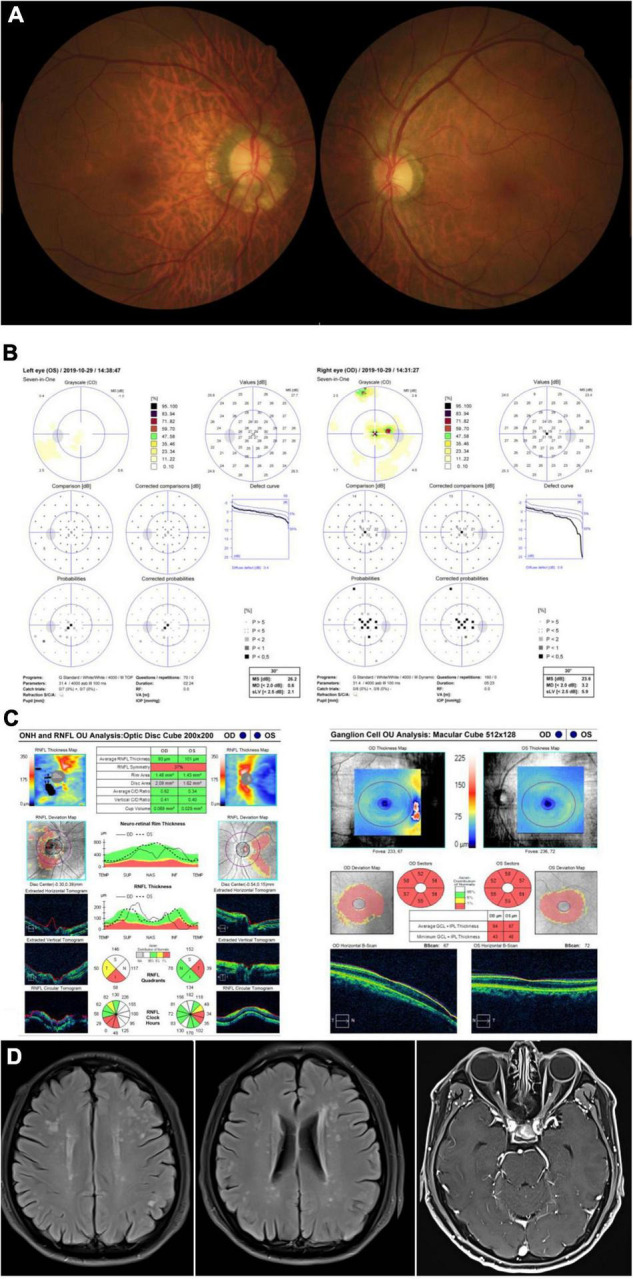
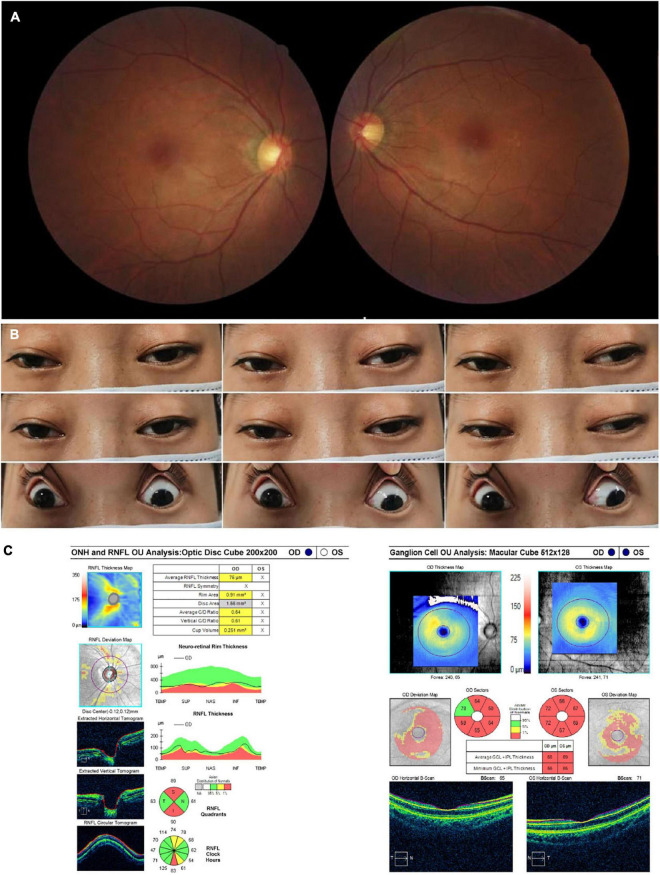
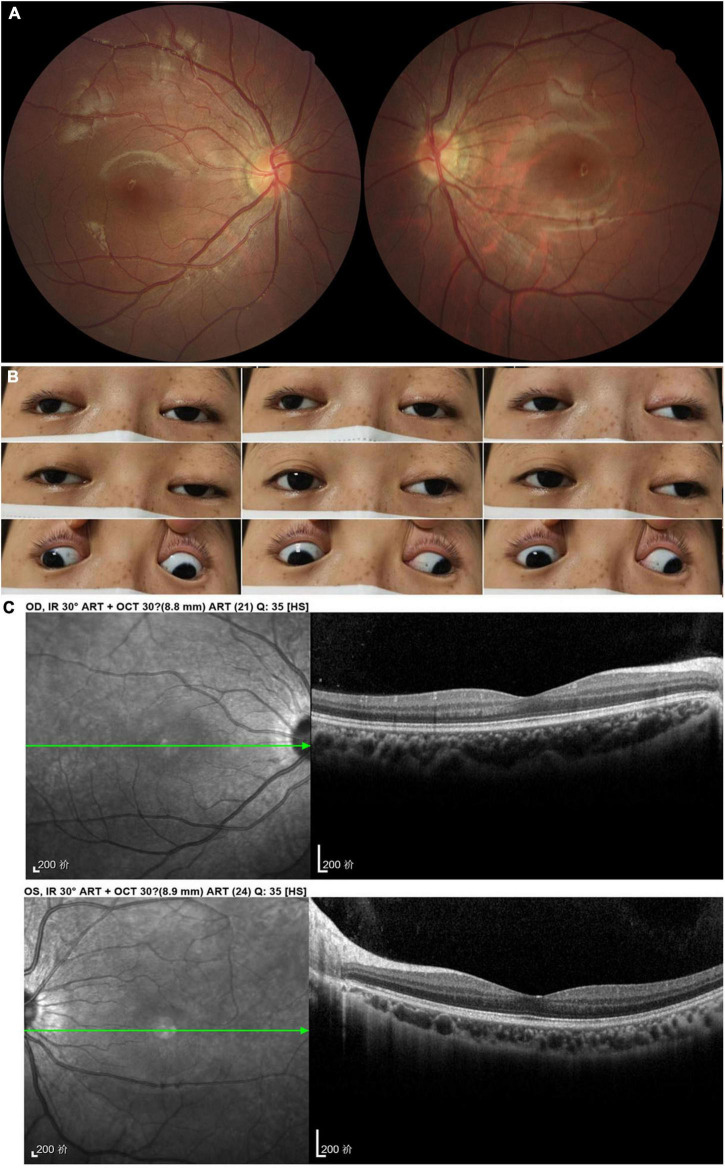
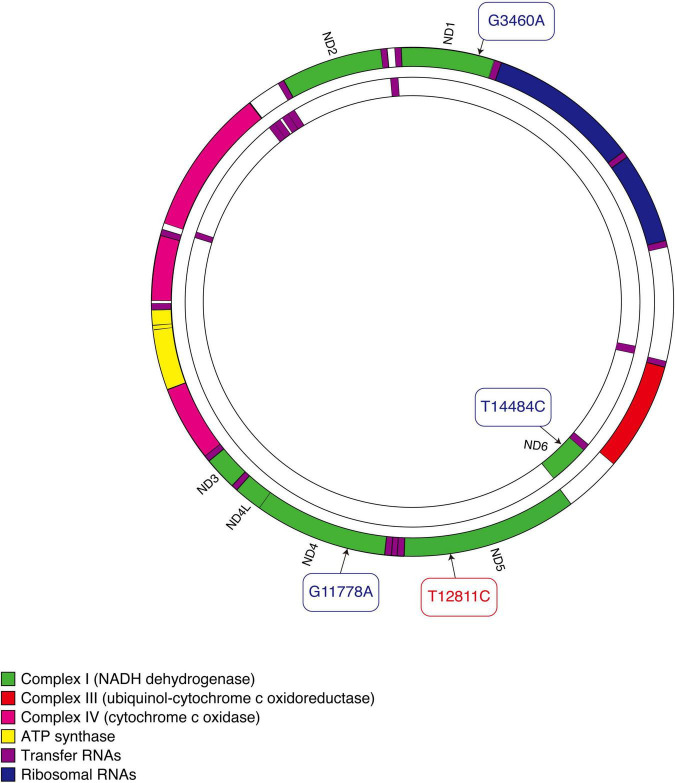
The T12811C mitochondrial DNA (mtDNA) mutation has been reported in Leber hereditary optic neuropathy (LHON) previously, with vision loss as the main manifestation. The involvement of other organ systems, including the central and peripheral nervous system, heart, and extraocular muscles, has not been well described. This case series report investigated four patients with T12811C mtDNA mutation, verified through a next generation sequencing. Two male patients presented with bilateral subacute visual decrease combined with involvement of multiple organ systems: leukoencephalopathy, hypertrophic cardiomyopathy, neurosensory deafness, spinal cord lesion and peripheral neuropathies. Two female patients presented with progressive ptosis and ophthalmoplegia, one of whom also manifested optic atrophy. This study found out that patients harboring T12811C mtDNA mutation manifested not only as vision loss, but also as a multi-system disorder affecting the nervous system, heart, and extraocular muscles.
Keywords: Leber hereditary optic neuropathy; mitochondrial DNA; mitochondrial disorder; ophthalmoplegia; optic atrophy.
Copyright © 2022 Xu, Sun, Feng, Chen, Sun, Chen and Tian.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Newman NJ, Wallace DC. Mitochondria and Leber’s hereditary optic neuropathy. Am J Ophthalmol. (1990) 109:726–30. - PubMed
Publication types
LinkOut - more resources
Full Text Sources