

Early evaluation of a next-generation surgical system in robot-assisted total laparoscopic hysterectomy: A prospective clinical cohort study
- PMID: 35861102
- PMCID: PMC9564672
- DOI: 10.1111/aogs.14407
Early evaluation of a next-generation surgical system in robot-assisted total laparoscopic hysterectomy: A prospective clinical cohort study
Abstract
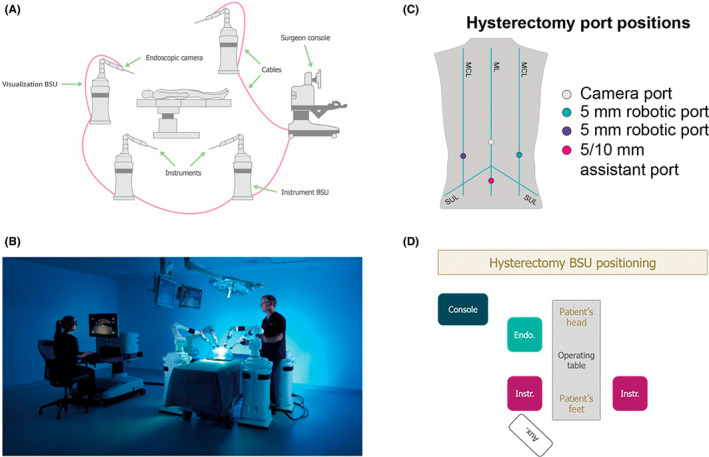
Introduction: This study aimed to demonstrate the safe and effective use of the Versius surgical system (CMR Surgical, Cambridge, UK) in robot-assisted total laparoscopic hysterectomy. This surgical robot was developed iteratively with input from surgeons to improve surgical outcomes and end-user experience. We report data from the gynecology cohort of an early clinical trial designed in broad alignment with IDEAL-D (Idea, Development, Exploration, Assessment, Long-term follow-up - Devices) stage 2b (Exploration).
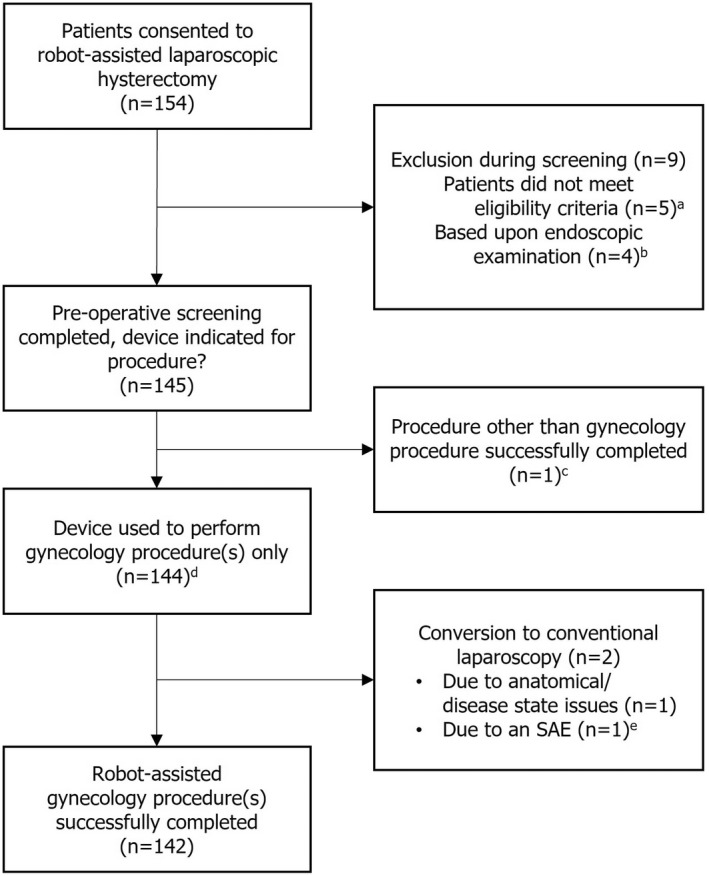
Material and methods: The study is registered in the Indian clinical trials register (CTRI/2019/02/017872). Adult women requiring total hysterectomy who provided informed consent and met the eligibility criteria underwent procedures at one of three hospitals in India. Five surgeons performed robot-assisted total laparoscopic hysterectomies using the device from March 2019 to September 2020. The primary endpoint was rate of unplanned conversion to conventional laparoscopic or open surgery. Adverse events were adjudicated by an independent clinical events committee using endoscope video recordings and clinical notes.
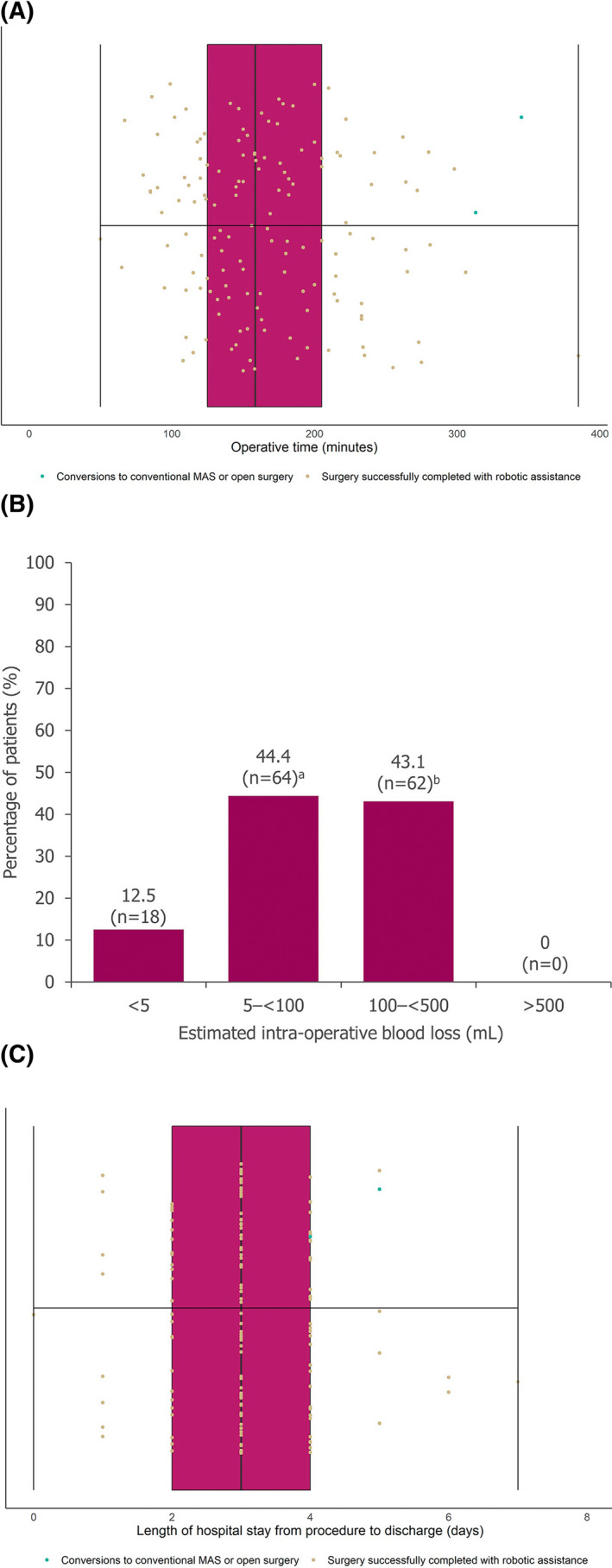
Results: In total, 144 women underwent surgery (median age: 44 years [range: 28-78]; median body mass index 25.8 kg/m2 [range: 14.3-47.8]). The rate of unplanned conversion to conventional laparoscopy was 2/144 (1.4%); neither conversion was device related. No surgery was converted to open. In total, 13 adverse events occurred among seven (4.9%) patients, comprising seven serious adverse events and six adverse events. One serious adverse event was deemed device-related. Two patients were readmitted to hospital within 30 days; both made a full recovery. No patients died within 90 days of surgery.
Conclusions: The device provides a safe and effective option for total laparoscopic hysterectomy; these findings support its continued implementation in larger patient cohorts and expansion in other major minimal access indications.
Keywords: clinical trial; gynecology; minimal access surgery; robot-assisted surgery; robotic surgical system; surgical robot.
© 2022 The Authors. Acta Obstetricia et Gynecologica Scandinavica published by John Wiley & Sons Ltd on behalf of Nordic Federation of Societies of Obstetrics and Gynecology (NFOG).
Conflict of interest statement
ED is a paid consultant for CMR Surgical, and MS is Chief Medical Officer and founder of CMR Surgical. The remaining authors have no conflicts of interest to declare.
Figures
Similar articles
-
Interim safety analysis of the first-in-human clinical trial of the Versius surgical system, a new robot-assisted device for use in minimal access surgery.Surg Endosc. 2021 Sep;35(9):5193-5202. doi: 10.1007/s00464-020-08014-4. Epub 2020 Sep 28. Surg Endosc. 2021. PMID: 32989548 Free PMC article. Clinical Trial.
-
An Early Prospective Clinical Study to Evaluate the Safety and Performance of the Versius Surgical System in Robot-Assisted Cholecystectomy.Ann Surg. 2023 Jan 1;277(1):9-17. doi: 10.1097/SLA.0000000000005410. Epub 2022 Feb 15. Ann Surg. 2023. PMID: 35170538 Free PMC article.
-
On-demand robotic surgery for hysterectomies: A combination of the best of robotic and laparoscopic approach.Womens Health (Lond). 2025 Jan-Dec;21:17455057251325029. doi: 10.1177/17455057251325029. Epub 2025 Mar 27. Womens Health (Lond). 2025. PMID: 40146923 Free PMC article.
-
Incidence and Prevention of Vaginal Cuff Dehiscence after Laparoscopic and Robotic Hysterectomy: A Systematic Review and Meta-analysis.J Minim Invasive Gynecol. 2021 Mar;28(3):710-720. doi: 10.1016/j.jmig.2020.12.016. Epub 2021 Jan 5. J Minim Invasive Gynecol. 2021. PMID: 33348012
-
[Robotic surgery in gynecology].Rozhl Chir. 2017 Winter;96(2):54-62. Rozhl Chir. 2017. PMID: 28429948 Review. Czech.
Cited by
-
Robot-assisted radical nephroureterectomy using the KangDuo Surgical Robot-01 System versus the da Vinci System: a multicenter prospective randomized controlled trial.Int Braz J Urol. 2024 Nov-Dec;50(6):727-736. doi: 10.1590/S1677-5538.IBJU.2024.0230. Int Braz J Urol. 2024. PMID: 39133792 Free PMC article. Clinical Trial.
-
A registry-based modified IDEAL stage 2b evaluation of urological procedures performed using the versius robotic surgical system.J Robot Surg. 2025 May 26;19(1):240. doi: 10.1007/s11701-025-02324-2. J Robot Surg. 2025. PMID: 40418458 Free PMC article.
-
The use of Versius CMR for pelvic surgery: a multicentric analysis of surgical setup and early outcomes.World J Urol. 2024 Jan 13;42(1):31. doi: 10.1007/s00345-023-04730-3. World J Urol. 2024. PMID: 38217724 Free PMC article.
-
Safe implementation of surgical innovation: a prospective registry of the Versius Robotic Surgical System.BMJ Surg Interv Health Technol. 2023 Feb 27;5(1):e000144. doi: 10.1136/bmjsit-2022-000144. eCollection 2023. BMJ Surg Interv Health Technol. 2023. PMID: 36865989 Free PMC article.
-
A retrospective analysis of robot-assisted total hysterectomy by transvaginal natural orifice transluminal endoscopic surgery.Heliyon. 2023 Aug 20;9(9):e19207. doi: 10.1016/j.heliyon.2023.e19207. eCollection 2023 Sep. Heliyon. 2023. PMID: 37662750 Free PMC article.
References
-
- He H, Zeng D, Ou H, Tang YZ, Li JJ, Zhong H. Laparoscopic treatment of endometrial cancer: systematic review. J Minim Invasive Gynecol. 2013;20:413‐423. - PubMed
-
- Xu T, Hutfless SM, Cooper MA, Zhou M, Massie AB, Makary MA. Hospital cost implications of increased use of minimally invasive surgery. JAMA Surg. 2015;150:489‐490. - PubMed
-
- Garcia‐Ruiz A, Gagner M, Miller JH, Steiner CP, Hahn JF. Manual vs robotically assisted laparoscopic surgery in the performance of basic manipulation and suturing tasks. Archives Surg. 1998;133:957‐961. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
