

TSH and FT4 Reference Intervals in Pregnancy: A Systematic Review and Individual Participant Data Meta-Analysis
- PMID: 35861700
- PMCID: PMC9516198
- DOI: 10.1210/clinem/dgac425
TSH and FT4 Reference Intervals in Pregnancy: A Systematic Review and Individual Participant Data Meta-Analysis
Abstract
Context: Interpretation of thyroid function tests during pregnancy is limited by the generalizability of reference intervals between cohorts due to inconsistent methodology.
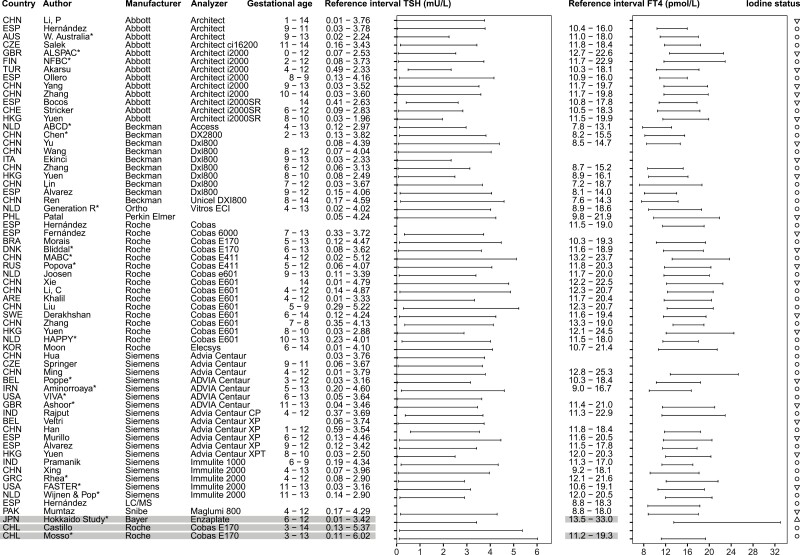
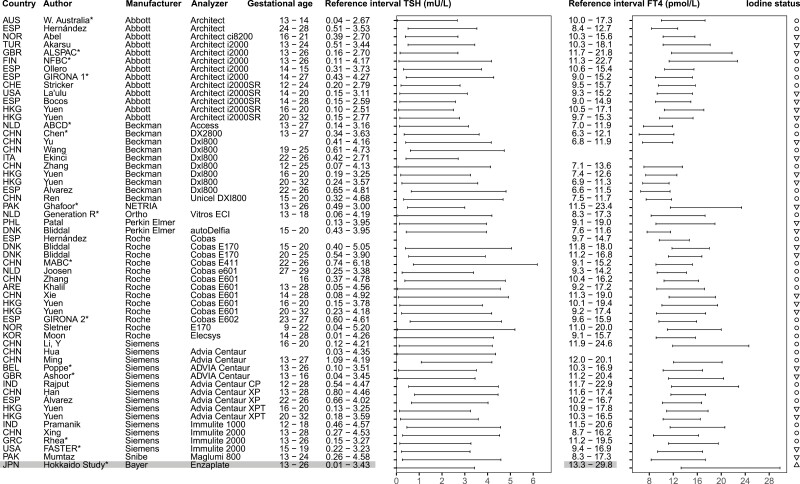
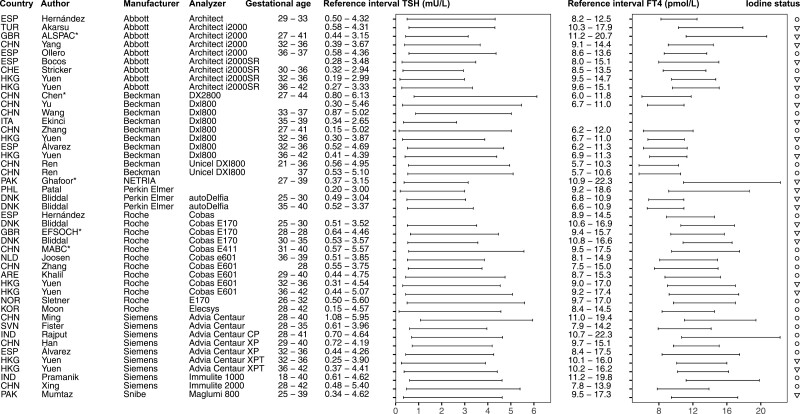
Objective: (1) To provide an overview of published reference intervals for thyrotropin (TSH) and free thyroxine (FT4) in pregnancy, (2) to assess the consequences of common methodological between-study differences by combining raw data from different cohorts.
Methods: (1) Ovid MEDLINE, EMBASE, and Web of Science were searched until December 12, 2021. Studies were assessed in duplicate. (2) The individual participant data (IPD) meta-analysis was performed in participating cohorts in the Consortium on Thyroid and Pregnancy.
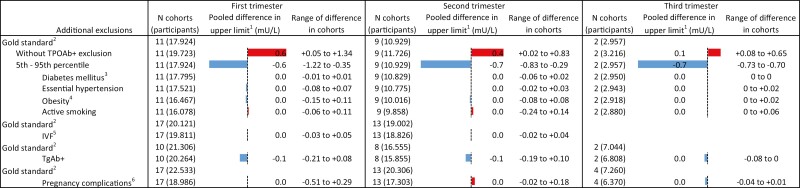
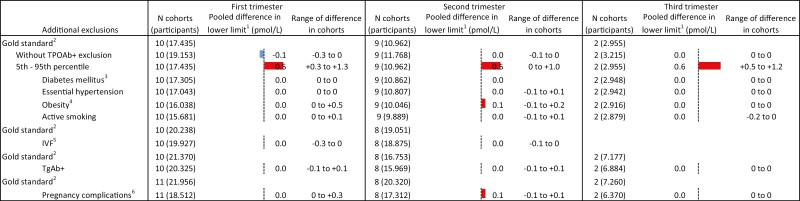
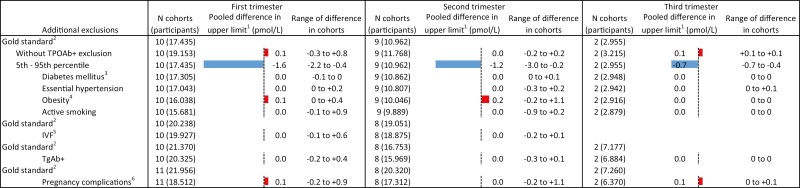
Results: (1) Large between-study methodological differences were identified, 11 of 102 included studies were in accordance with current guidelines; (2) 22 cohorts involving 63 198 participants were included in the meta-analysis. Not excluding thyroid peroxidase antibody-positive participants led to a rise in the upper limits of TSH in all cohorts, especially in the first (mean +17.4%; range +1.6 to +30.3%) and second trimester (mean +9.8%; range +0.6 to +32.3%). The use of the 95th percentile led to considerable changes in upper limits, varying from -10.8% to -21.8% for TSH and -1.2% to -13.2% for FT4. All other additional exclusion criteria changed reference interval cut-offs by a maximum of 3.5%. Applying these findings to the 102 studies included in the systematic review, 48 studies could be used in a clinical setting.
Conclusion: We provide an overview of clinically relevant reference intervals for TSH and FT4 in pregnancy. The results of the meta-analysis indicate that future studies can adopt a simplified study setup without additional exclusion criteria.
Keywords: free thyroxine (FT4); pregnancy; reference values; thyroid; thyrotropin (TSH).
© The Author(s) 2022. Published by Oxford University Press on behalf of the Endocrine Society.
Figures
References
-
- Negro R, Stagnaro-Green A. Diagnosis and management of subclinical hypothyroidism in pregnancy. BMJ. 2014;349:g4929. - PubMed
-
- Alexander EK, Pearce EN, Brent GA, et al. . 2017 Guidelines of the American Thyroid Association for the Diagnosis and Management of Thyroid Disease During Pregnancy and the Postpartum. Thyroid. 2017;27(3):315-389. - PubMed
-
- Hershman JM. The role of human chorionic gonadotropin as a thyroid stimulator in normal pregnancy. J Clin Endocr Metab. 2008;93(9):3305-3306. - PubMed
