

Left Ventricular Strain Analysis During Submaximal Semisupine Bicycle Exercise Stress Echocardiography in Childhood Cancer Survivors
- PMID: 35861837
- PMCID: PMC9707818
- DOI: 10.1161/JAHA.122.025324
Left Ventricular Strain Analysis During Submaximal Semisupine Bicycle Exercise Stress Echocardiography in Childhood Cancer Survivors
Abstract
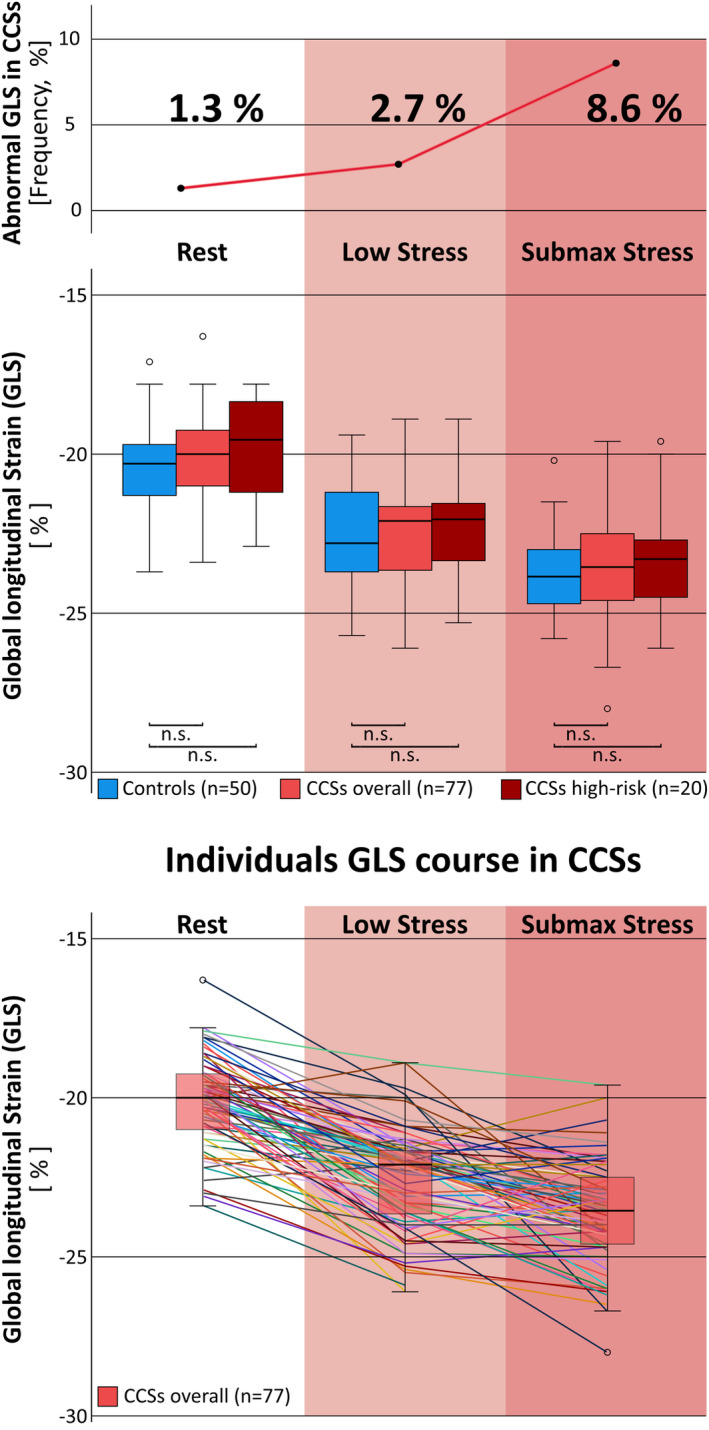
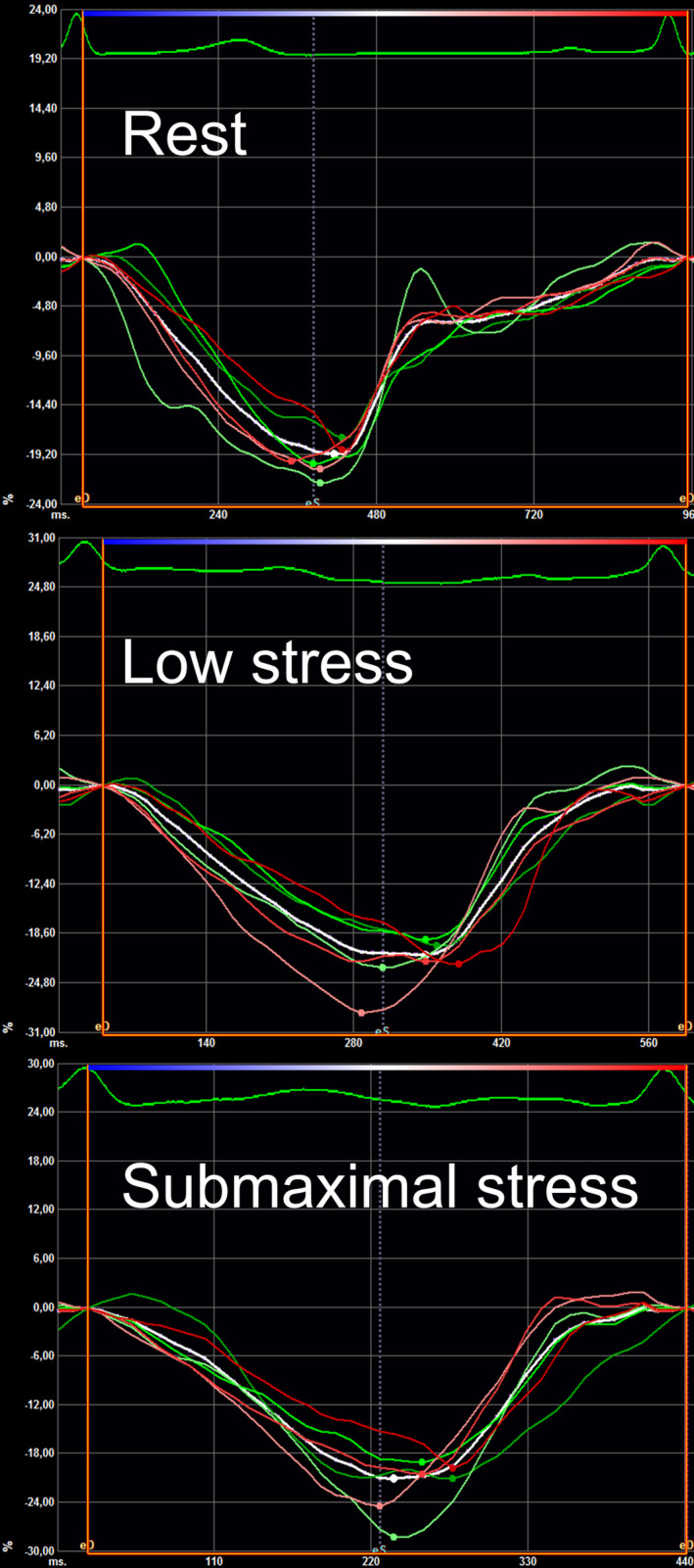
Background Childhood cancer survivors (CCSs) show relevant cardiac morbidity and mortality throughout life. Early detection is key for optimal support of patients at risk. The aim of this study was to evaluate 2-dimensional speckle-tracking echocardiography strain analysis during semisupine exercise stress in CCSs for detection of subclinical left ventricular dysfunction after cancer treatment. Methods and Results Seventy-seven CCSs ≥1-year postchemotherapy were prospectively examined at rest, low, and submaximal stress level and compared with a cohort of healthy adolescents and young adults (n=50). Global longitudinal strain (GLS), short axis circumferential strain, and corresponding strain rates were analyzed using vendor-independent software. CCSs at median 7.8 years postchemotherapy showed comparable left ventricular GLS, circumferential strain, and strain rate values at all stress stages to healthy controls. Yet, prevalence of abnormal GLS (defined as <2 SD of controls reference) in CCSs was 1.3% at rest, 2.7% at low, and 8.6% at submaximal stress. In CCSs, relative change of circumferential strain from rest to submaximal stress was lower than in healthy controls, median 16.9 (interquartile range [IQR], 3.4; 28.8) % versus 23.3 (IQR, 11.3; 33.3) %, P=0.03, most apparent in the subgroups of CCSs after high-dose anthracycline treatment and cancer diagnosis before the age of 5 years. Conclusions In this prospective 2-dimensional speckle tracking echocardiography strain study, prevalence of abnormal left ventricular GLS increased with stress level reflecting impaired cardiac adaptation to exercise stress in some CCSs. However, relatively early after last chemotherapy, this did not result in significant differences of mean GLS-, circumferential strain-, and strain rate values between CCSs and controls at any stress level.
Keywords: 2D‐speckle‐tracking strain echocardiography; cardio‐oncology; childhood cancer survivor; stress echocardiography.
Figures
References
-
- Mulrooney DA, Yeazel MW, Kawashima T, Mertens AC, Mitby P, Stovall M, Donaldson SS, Green DM, Sklar CA, Robison LL, et al. Cardiac outcomes in a cohort of adult survivors of childhood and adolescent cancer: retrospective analysis of the childhood cancer survivor study cohort. BMJ. 2009;339:b4606. doi: 10.1136/bmj.b4606 - DOI - PMC - PubMed
-
- Plana JC, Galderisi M, Barac A, Ewer MS, Ky B, Scherrer‐Crosbie M, Ganame J, Sebag IA, Agler DA, Badano LP, et al. Expert consensus for multimodality imaging evaluation of adult patients during and after cancer therapy: a report from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging. 2014;15:1063–1093. doi: 10.1093/ehjci/jeu192 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
