

Keratoameloblastoma: A Report of Seven New Cases and Review of Literature
- PMID: 35861917
- PMCID: PMC9729669
- DOI: 10.1007/s12105-022-01470-5
Keratoameloblastoma: A Report of Seven New Cases and Review of Literature
Abstract
Background: Keratoameloblastoma (KA) is an uncommon and controversial variant of ameloblastoma exhibiting central keratinisation. Due to their rarity, there is limited information in the literature on their clinical, radiologic and histologic features. This study adds seven additional cases of KA to the literature, and reviews the current published literature on this rare entity.
Methods: KAs were retrospectively reviewed over a 20-year period from three Oral and Maxillofacial Pathology Laboratories. Included cases were examined and the diagnosis confirmed under conventional microscopy. Immunohistochemistry with the use of a monoclonal antibody against calretinin was performed on included cases. The clinical, radiologic and histologic features of the seven new cases of KA were analysed and compared to existing cases in the literature.
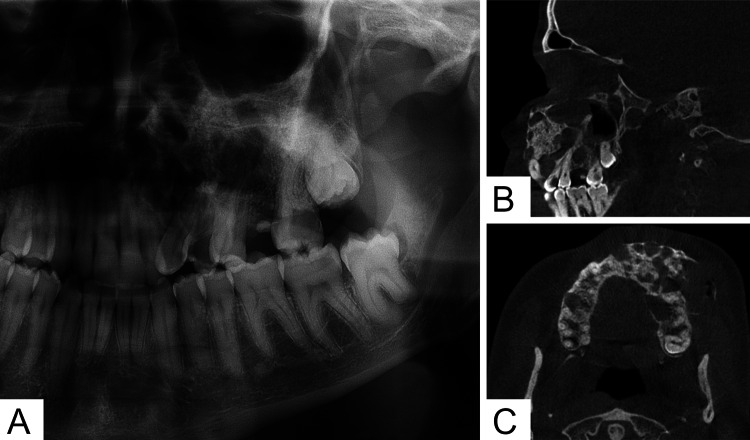
Results: KAs presented at a mean age of 40 years with a nearly equal gender distribution and a mandibular predilection (65%). The majority (92%) of cases presented with localised swelling with associated pain in 32% of cases. Mixed density or internal calcifications were noted in 40% of cases. All tumours presented with bony expansion, with cortical destruction noted in 62% of cases. Histologically, all tumours consisted of solid and cystic follicles with surface parakeratinisation and lamellated accumulations of central keratin. In areas the cystic follicles had an epithelial lining suggestive of an OKC. There were focal luminal areas of loosely arranged polygonal cells reminiscent of the stellate reticulum. The basal cells consisted of columnar cells with evidence of palisading and prominent subnuclear vacuolisation. Of the cases treated via tumour resection, 27% presented with tumour recurrence.
Conclusion: This case series reports seven additional cases of KA, taking the total to 26 reported cases. The identification of subtle histologic features, including focal stellate reticulum-like central areas, subnuclear vacuolisation and lamellated-type central keratinisation, are key in diagnosing KA. The radiologic features will often indicate signs of aggressiveness such as cortical destruction, differentiating KA from OKC. All cases were completely negative for calretinin IHC, limiting its use in distinguishing KA from OKC. Further large series are needed to expand the current understanding of this rare variant of ameloblastoma.
Keywords: Ameloblastoma; Immunohistochemistry; Keratoameloblastoma; Molecular pathology; Odontogenic keratocyst; Odontogenic tumour.
© 2022. The Author(s), under exclusive licence to Springer Science+Business Media, LLC, part of Springer Nature.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures


References
-
- Brierley DJ, Hunter KD. Odontogenic tumours. Diagn Histopathol. 2015;21(9):370–379. doi: 10.1016/j.mpdhp.2015.07.003. - DOI
-
- El-Naggar AK, Chan JKC, Rubin Grandis J, Takata T, Slootweg PJ. WHO classification of head and neck tumours. World Health Organization Classification of tumours. 4. Lyon: International Agency for Research on Cancer; 2017.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
