

Vital Signs: Drug Overdose Deaths, by Selected Sociodemographic and Social Determinants of Health Characteristics - 25 States and the District of Columbia, 2019-2020
- PMID: 35862289
- PMCID: PMC9310633
- DOI: 10.15585/mmwr.mm7129e2
Vital Signs: Drug Overdose Deaths, by Selected Sociodemographic and Social Determinants of Health Characteristics - 25 States and the District of Columbia, 2019-2020
Abstract
Introduction: Drug overdose deaths increased approximately 30% from 2019 to 2020 in the United States. Examining rates by demographic and social determinants of health characteristics can identify disproportionately affected populations and inform strategies to reduce drug overdose deaths.
Methods: Data from the State Unintentional Drug Overdose Reporting System (SUDORS) were used to analyze overdose death rates from 2019 to 2020 in 25 states and the District of Columbia. Rates were examined by race and ethnicity and county-level social determinants of health (e.g., income inequality and treatment provider availability).
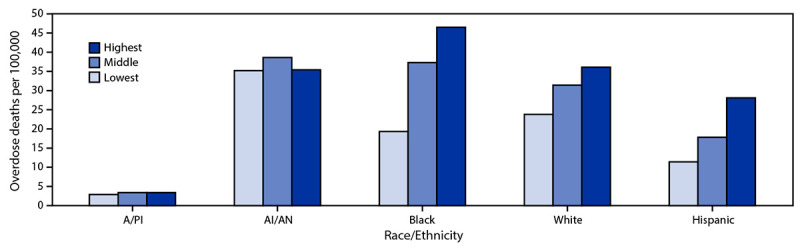
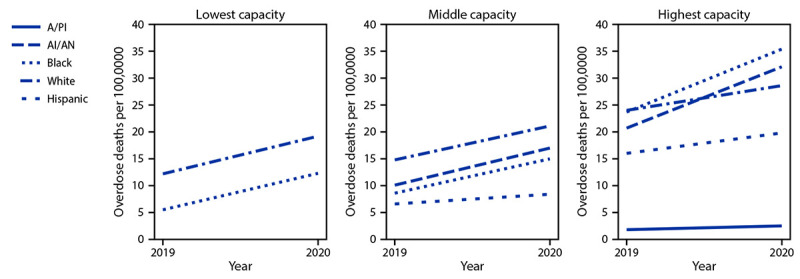
Results: From 2019 to 2020, drug overdose death rates increased by 44% and 39% among non-Hispanic Black (Black) and non-Hispanic American Indian or Alaska Native (AI/AN) persons, respectively. Significant disparities were found across sex, age, and racial and ethnic subgroups. In particular, the rate in 2020 among Black males aged ≥65 years (52.6 per 100,000) was nearly seven times that of non-Hispanic White males aged ≥65 years (7.7). A history of substance use was frequently reported. Evidence of previous substance use treatment was lowest for Black persons (8.3%). Disparities in overdose deaths, particularly among Black persons, were larger in counties with greater income inequality. Opioid overdose rates in 2020 were higher in areas with more opioid treatment program availability compared with areas with lower opioid treatment availability, particularly among Black (34.3 versus 16.6) and AI/AN (33.4 versus 16.2) persons.
Conclusions and implications for public health practice: Health disparities in overdose rates continue to worsen, particularly among Black and AI/AN persons; social determinants of health, such as income inequality, exacerbate these inequities. Implementation of available, evidence-based, culturally responsive overdose prevention and response efforts that address health disparities impacting disproportionately affected populations are urgently needed.
Conflict of interest statement
All authors have completed and submitted the International Committee of Medical Journal Editors form for disclosure of potential conflicts of interest. No potential conflicts of interest were disclosed.
Figures
References
-
- Hedegaard H, Miniño AM, Spencer MR, Warner M. Drug overdose deaths in the United States, 1999–2020. NCHS data brief, no. 428. Hyattsville, MD: US Department of Health and Human Services, CDC, National Center for Health Statistics; 2021. 10.15620/cdc:112340 - DOI
