

Phenotypic Heterogeneity of Fulminant COVID-19--Related Myocarditis in Adults
- PMID: 35863846
- PMCID: PMC9291241
- DOI: 10.1016/j.jacc.2022.04.056
Phenotypic Heterogeneity of Fulminant COVID-19--Related Myocarditis in Adults
Abstract
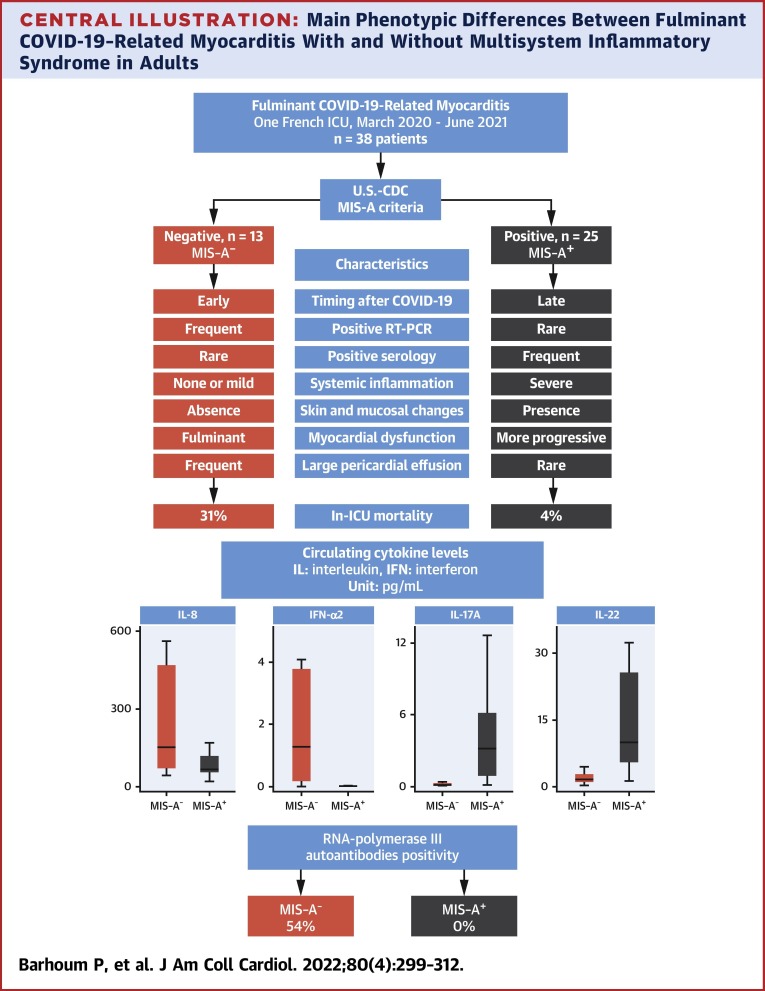
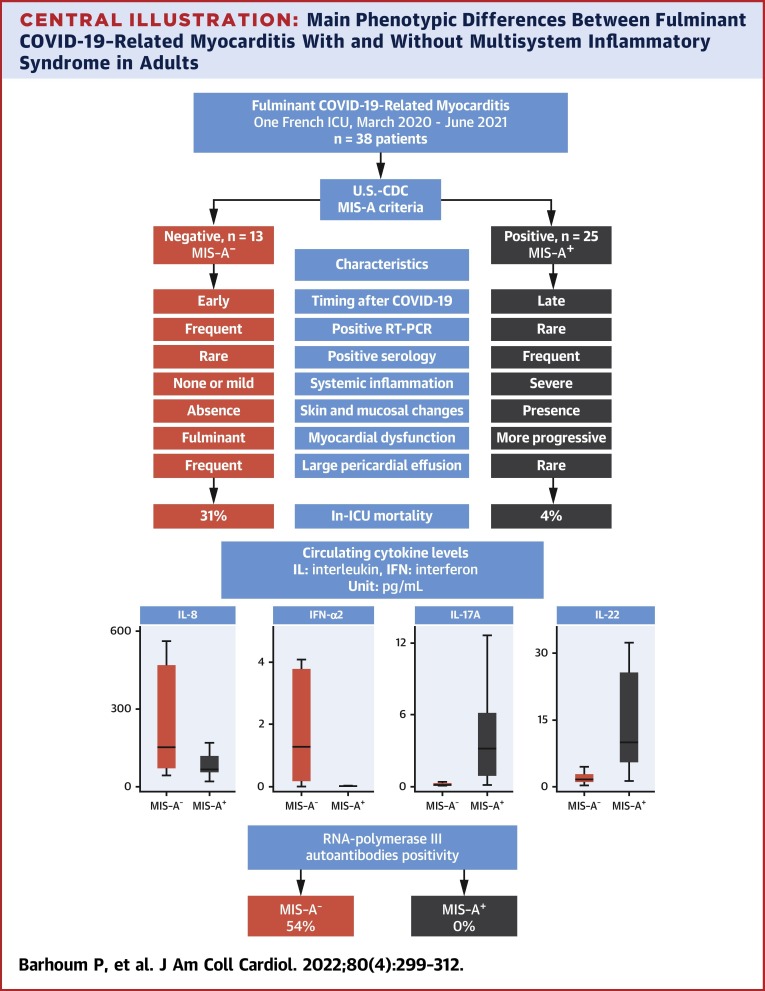
Background: Adults who have been infected with SARS-CoV-2 can develop a multisystem inflammatory syndrome (MIS-A), including fulminant myocarditis. Yet, several patients fail to meet MIS-A criteria, suggesting the existence of distinct phenotypes in fulminant COVID-19-related myocarditis.
Objectives: This study sought to compare the characteristics and clinical outcome between patients with fulminant COVID-19-related myocarditis fulfilling MIS-A criteria (MIS-A+) or not (MIS-A-).
Methods: A monocentric retrospective analysis of consecutive fulminant COVID-19-related myocarditis in a 26-bed intensive care unit (ICU).
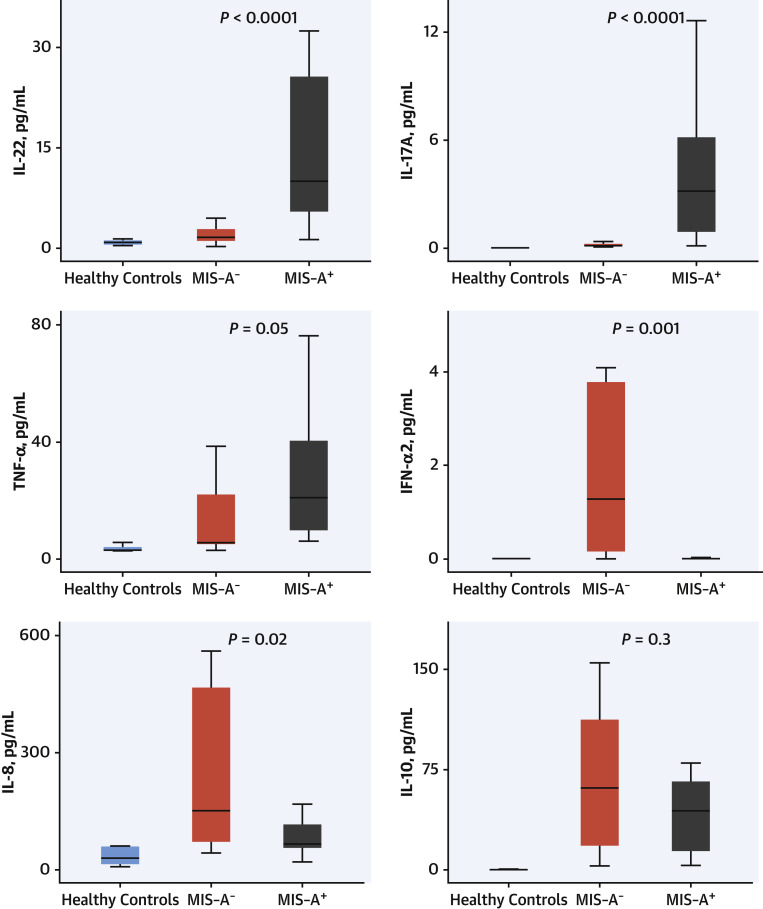
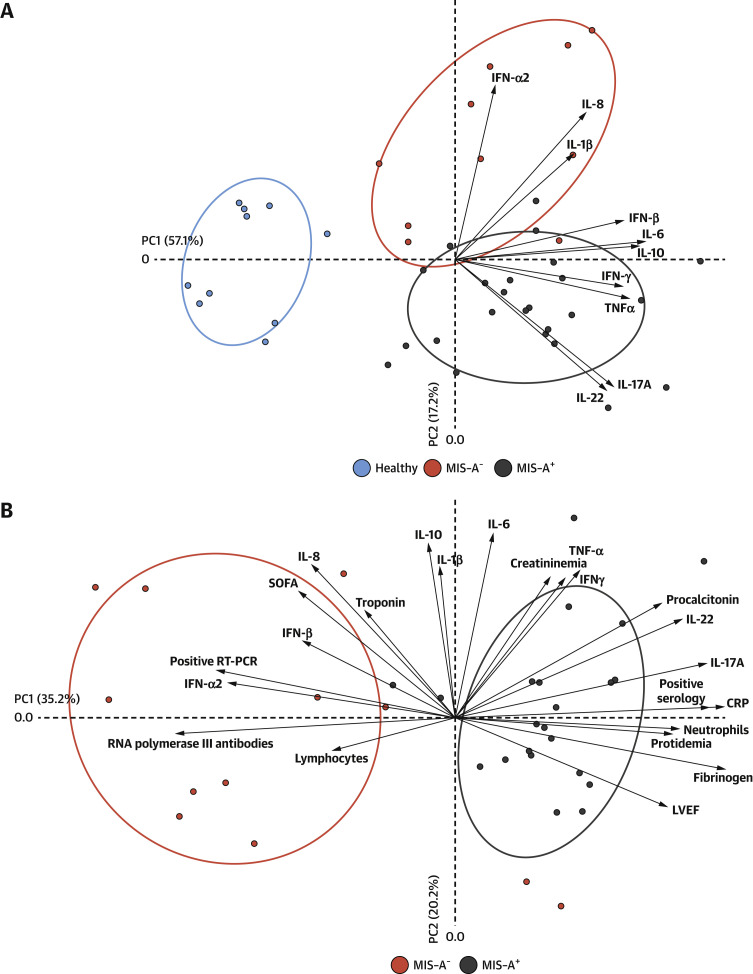
Results: Between March 2020 and June 2021, 38 patients required ICU admission (male 66%; mean age 32 ± 15 years) for suspected fulminant COVID-19-related myocarditis. In-ICU treatment for organ failure included dobutamine 79%, norepinephrine 60%, mechanical ventilation 50%, venoarterial extracorporeal membrane oxygenation 42%, and renal replacement therapy 29%. In-hospital mortality was 13%. Twenty-five patients (66%) met the MIS-A criteria. MIS-A- patients compared with MIS-A+ patients were characterized by a shorter delay between COVID-19 symptoms onset and myocarditis, a lower left ventricular ejection fraction, and a higher rate of in-ICU organ failure, and were more likely to require mechanical circulatory support with venoarterial extracorporeal membrane oxygenation (92% vs 16%; P < 0.0001). In-hospital mortality was higher in MIS-A- patients (31% vs 4%). MIS-A+ had higher circulating levels of interleukin (IL)-22, IL-17, and tumor necrosis factor-α (TNF-α), whereas MIS-A- had higher interferon-α2 (IFN-α2) and IL-8 levels. RNA polymerase III autoantibodies were present in 7 of 13 MIS-A- patients (54%) but in none of the MIS-A+ patients.
Conclusion: MIS-A+ and MIS-A- fulminant COVID-19-related myocarditis patients have 2 distinct phenotypes with different clinical presentations, prognosis, and immunological profiles. Differentiating these 2 phenotypes is relevant for patients' management and further understanding of their pathophysiology.
Keywords: COVID-19; RNA polymerase III autoantibodies; SARS-CoV-2; VA-ECMO; cytokines; fulminant myocarditis; multisystem inflammatory syndrome.
Copyright © 2022 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures This study was supported by the Fondation de France, ‘‘Tous unis contre le virus’’ framework Alliance (Fondation de France, AP-HP, Institut Pasteur) in collaboration with Agence Nationale de la Recherche (ANR Flash COVID19 program), by the SARS-CoV-2 Program of the Faculty of Medicine from Sorbonne University ICOViD programs, by the Programme Hospitalier de Recherche Clinique PHRC-20-0375 COVID-19 (principal investigator D Gorochov). The authors declare that a patent application has been filed on these results. Dr Pineton de Chambrun was supported for this study by a grant from la Société Française Nationale de Médecine Interne (SNFMI-2021). Dr Pineton de Chambrun has received a research grant from Octapharma; and has received lecture fees from Sanofi. Dr Kerneis has received research grants from the Fédération Française de Cardiologie, French Ministry of Health; and has received consulting fees from Bayer, Sanofi, and Kiniksa. Dr Montalescot has received research grants from Abbott, Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Boston Scientific, Bristol Myers Squibb, Cell Prothera, CSL Behring, Europa, Idorsia, IRIS-Servier, Medtronic, Merck Sharp and Dohme, Novartis, Pfizer, Quantum Genomics, and Sanofi. Dr Combes has received grants and personal fees from Maquet, Xenios, and Baxter outside the submitted work. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
COVID-19-Associated Fulminant Myocarditis: Pathophysiology-Related Phenotypic Variance.J Am Coll Cardiol. 2022 Jul 26;80(4):313-315. doi: 10.1016/j.jacc.2022.06.003. J Am Coll Cardiol. 2022. PMID: 35863847 Free PMC article.
References
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
