

The efficacy of topical sucralfate in improving pain and wound healing after haemorrhoidectomy procedure: A systematic review, meta-analysis, and meta-regression of randomised clinical trials
- PMID: 35864080
- PMCID: PMC9885481
- DOI: 10.1111/iwj.13901
The efficacy of topical sucralfate in improving pain and wound healing after haemorrhoidectomy procedure: A systematic review, meta-analysis, and meta-regression of randomised clinical trials
Abstract
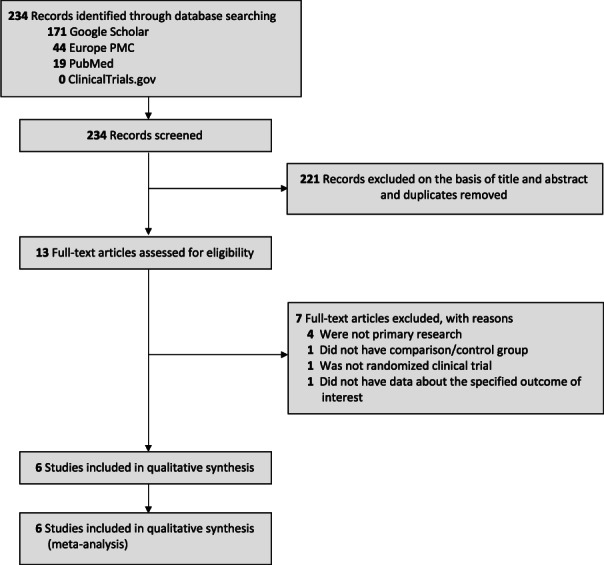
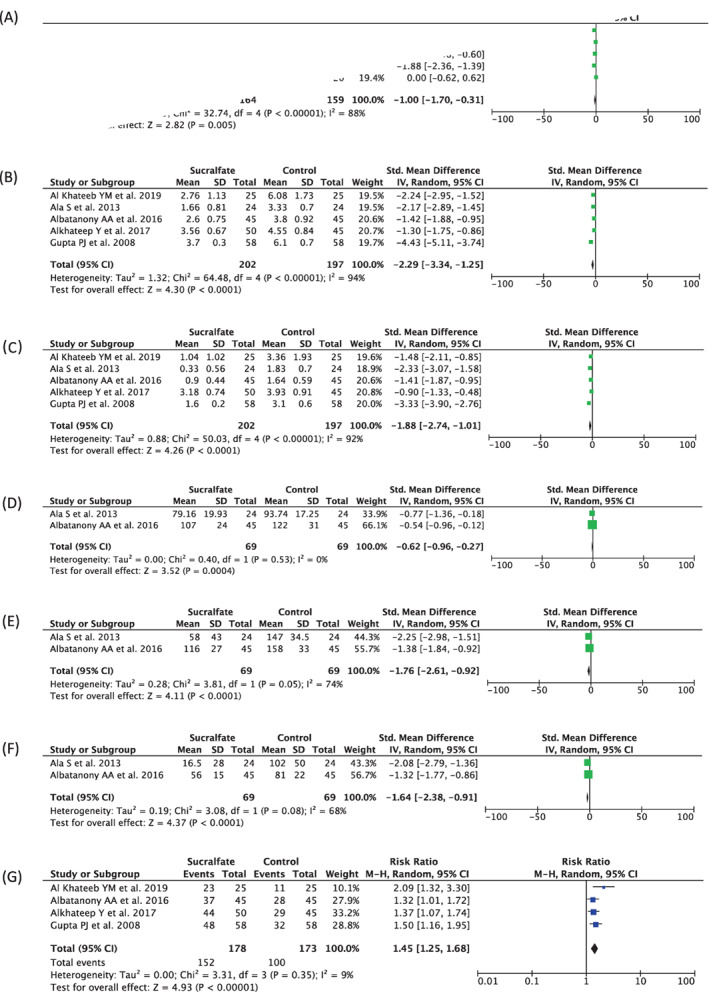
Pain and wound after haemorrhoidectomy constantly bothered the patient's convenience. Recurrently, topical sucralfate is used to treat excoriations and burns. It is considered to enhance epidermal growth and tissue granulation, thus, alleviating patients' problems. This study evaluated topical sucralfate's feasibility, safety, and superiority after haemorrhoidectomy. We searched randomised controlled trial (RCT) studies in PubMed, Google Scholar, Europe PMC, and ClinicalTrials.gov until March 29th, 2022. We investigated the influence of topical sucralfate on pain score postoperatively (24 hours, 7 days, and 14 days), pethidine usage, diclofenac usage, and wound healing rate compared to placebo. This study was conducted following the PRISMA guidelines. This study sorted the final six studies with 439 patients underwent haemorrhoidectomy. Topical sucralfate demonstrated significant outcomes on VAS 24 hours post-operative [Std. Mean Difference -1.00 (95% CI -1.70, -0.31), P = .005], VAS 7 days post-operative [Std. Mean Difference -2.29 (95% CI -3.34, -1.25), P < .0001], VAS 14 days post-operative [Std. Mean Difference -1.88 (95% CI -2.74, -1.01), P < .0001], pethidine usage within 24 hours post-operative [Std. Mean Difference -0.62 (95% CI -0.96, -0.27), P = .0004], diclofenac usage 7 days post-operative [Std. Mean Difference -1.76 (95% CI -2.61, -0.92), P < .0001], diclofenac usage 14 days post-operative [Std. Mean Difference -1.64 (95% CI -2.38, -0.91), P < .0001], and wound healing rate at 28-day post-operative [RR 1.45 (95% CI 1.25-1.68), P < .00001]. Topical sucralfate alleviated pain, improved wound healing, and minimised the usage of pethidine and diclofenac compared to placebo.
Keywords: haemorrhoidectomy; pain; systematic review; topical sucralfate; wound healing.
© 2022 The Authors. International Wound Journal published by Medicalhelplines.com Inc (3M) and John Wiley & Sons Ltd.
Conflict of interest statement
The authors have no conflict of interest to declare.
Figures
Similar articles
-
Evaluation of the efficacy of topical sucralfate on healing haemorrhoidectomy incision wounds and reducing pain severity: A randomised clinical trial.Int Wound J. 2020 Aug;17(4):1047-1051. doi: 10.1111/iwj.13369. Epub 2020 Apr 21. Int Wound J. 2020. PMID: 32319175 Free PMC article. Clinical Trial.
-
Topical analgesia following excisional haemorrhoidectomy: a systematic review and meta-analysis of randomised controlled trials.Int J Colorectal Dis. 2020 Feb;35(2):181-197. doi: 10.1007/s00384-019-03497-7. Epub 2020 Jan 2. Int J Colorectal Dis. 2020. PMID: 31897645
-
Topical sucralfate decreases pain after hemorrhoidectomy and improves healing: a randomized, blinded, controlled study.Dis Colon Rectum. 2008 Feb;51(2):231-4. doi: 10.1007/s10350-007-9092-4. Epub 2007 Dec 18. Dis Colon Rectum. 2008. PMID: 18095028 Clinical Trial.
-
Metronidazole following excisional haemorrhoidectomy: a systematic review and meta-analysis.ANZ J Surg. 2018 May;88(5):408-414. doi: 10.1111/ans.14236. Epub 2018 Mar 23. ANZ J Surg. 2018. PMID: 29573108
-
Efficacy of 10% sucralfate ointment after anal fistulotomy: A prospective, double-blind, randomized, placebo-controlled trial.Int J Surg. 2016 Dec;36(Pt A):13-17. doi: 10.1016/j.ijsu.2016.10.017. Epub 2016 Oct 17. Int J Surg. 2016. PMID: 27765686 Clinical Trial.
Cited by
-
Effectiveness and tolerability of rectal ointment and suppositories containing sucralfate for hemorrhoidal symptoms: a prospective, observational study.Int J Colorectal Dis. 2024 May 16;39(1):72. doi: 10.1007/s00384-024-04642-7. Int J Colorectal Dis. 2024. PMID: 38750150 Free PMC article.
-
Clinical Trial: Precise Administration of Sucralfate Powder in Prevention of Delayed Postpolypectomy Bleeding. A Randomized Controlled Trial.Clin Transl Gastroenterol. 2025 Apr 1;16(4):e00818. doi: 10.14309/ctg.0000000000000818. Clin Transl Gastroenterol. 2025. PMID: 39836033 Free PMC article. Clinical Trial.
-
Comparison of ointment-based agents after excisional procedures for hemorrhoidal disease: a network meta-analysis of randomized controlled trials.Langenbecks Arch Surg. 2023 Oct 14;408(1):401. doi: 10.1007/s00423-023-03128-4. Langenbecks Arch Surg. 2023. PMID: 37837466
References
-
- Sheikh P, Régnier C, Goron F, Salmat G. The prevalence, characteristics and treatment of hemorrhoidal disease: results of an international web‐based survey. J Compar Effective Res. 2020;9(17):1219‐1232. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
