

Chronic wounds
- PMID: 35864102
- PMCID: PMC10352385
- DOI: 10.1038/s41572-022-00377-3
Chronic wounds
Abstract
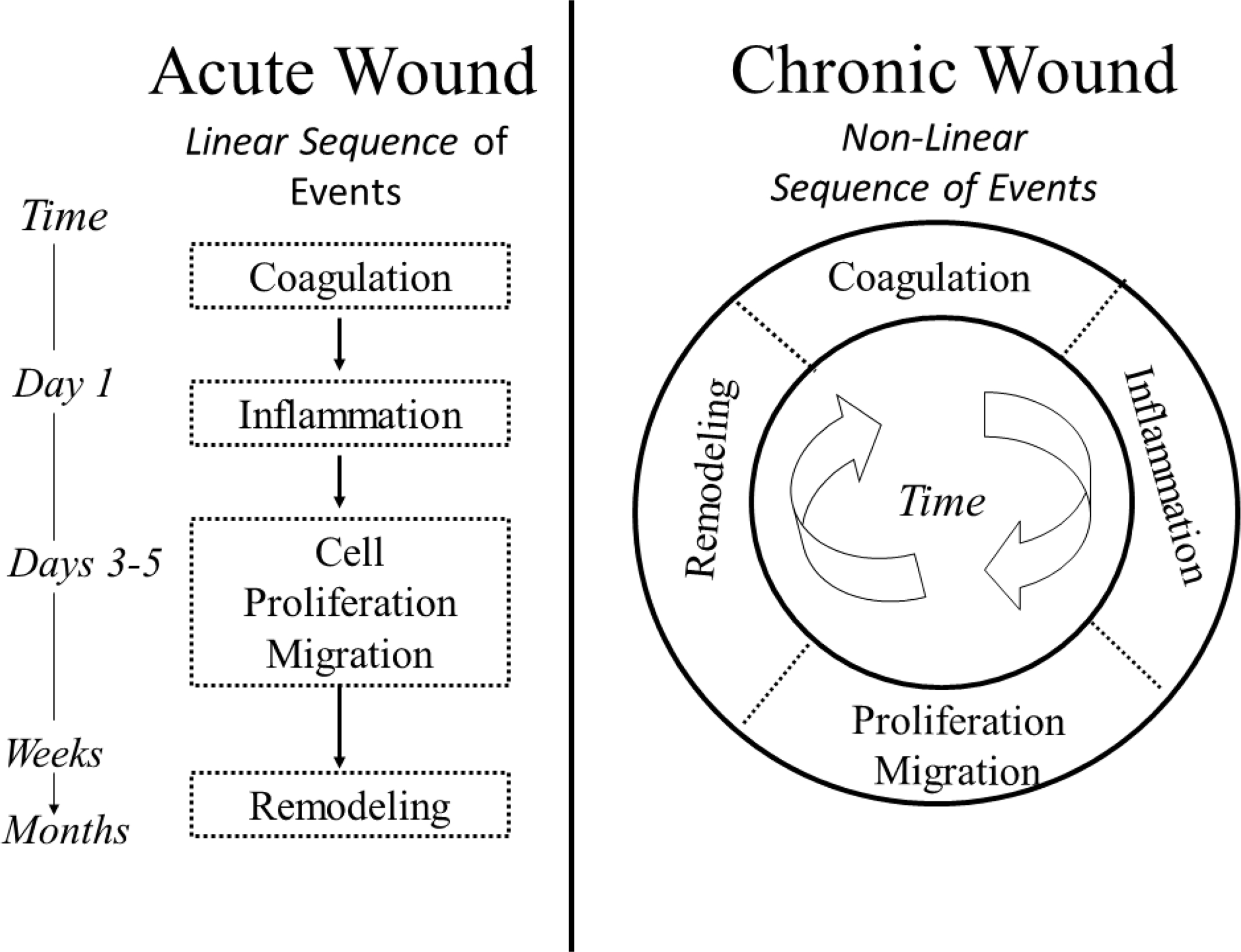
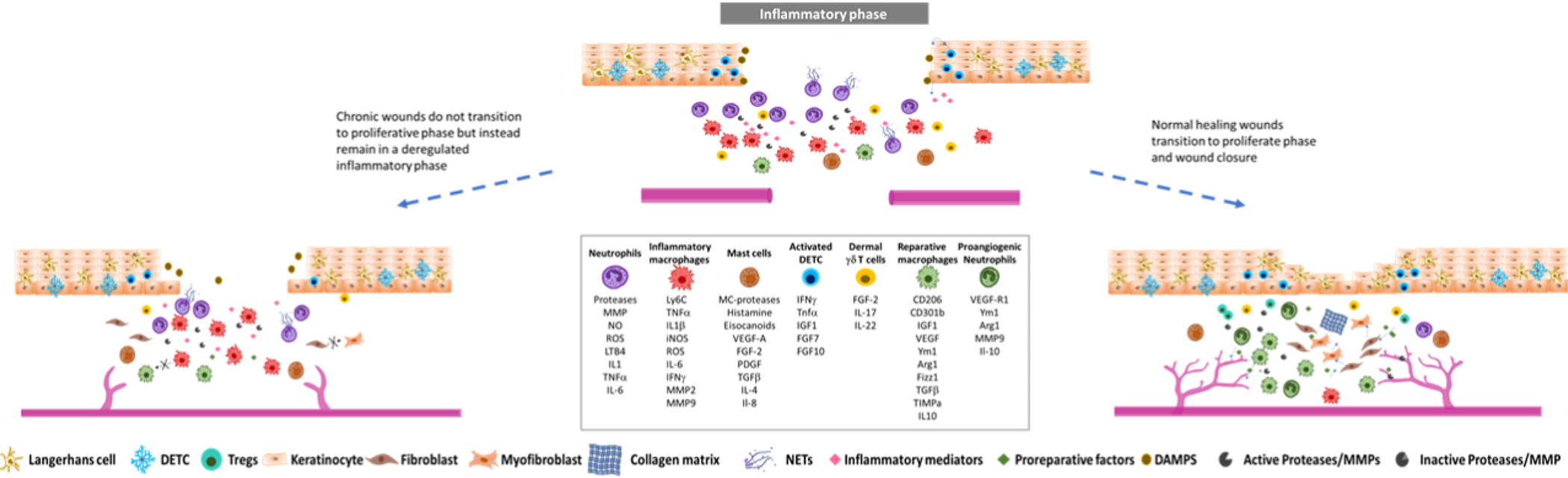
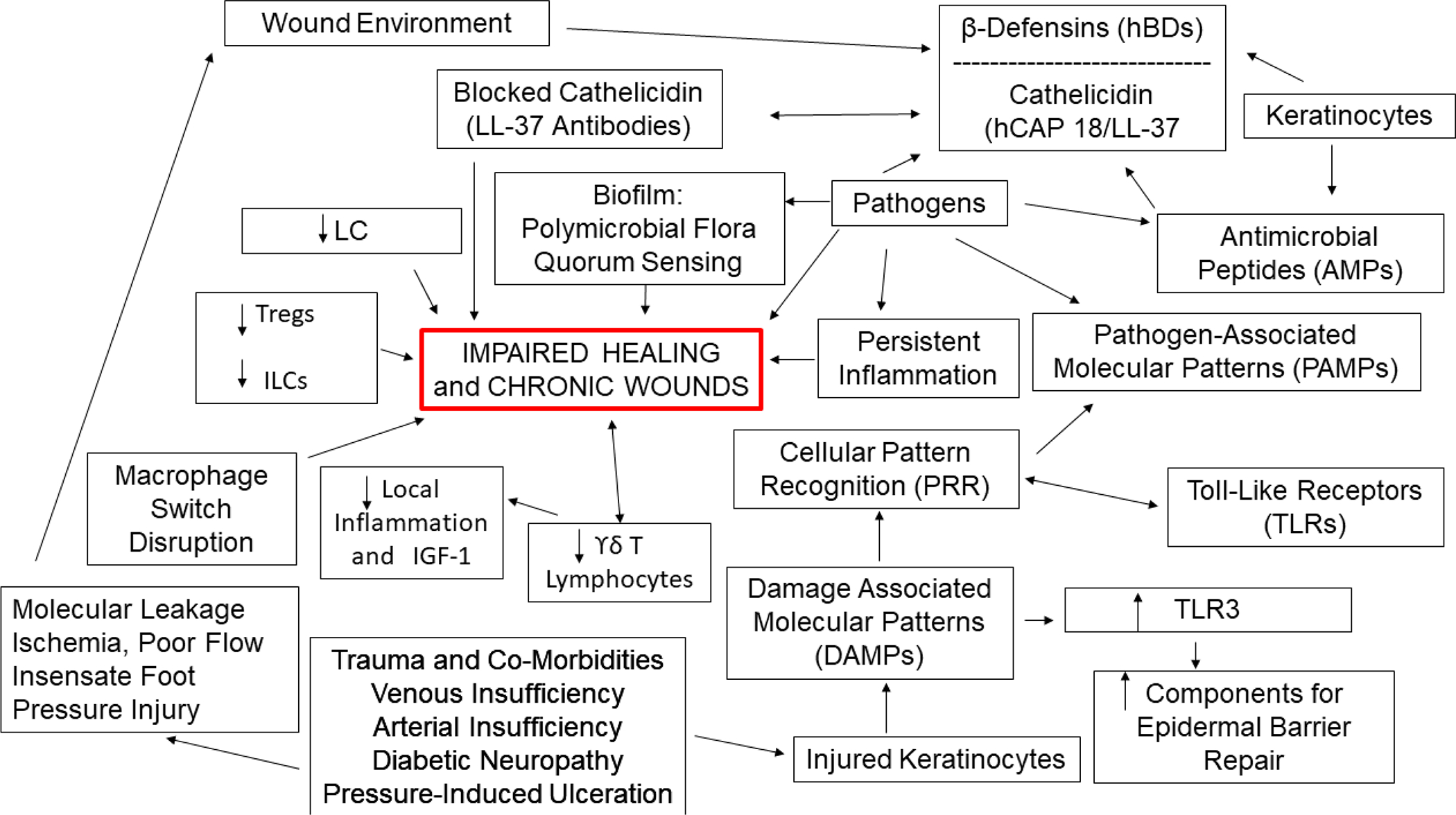
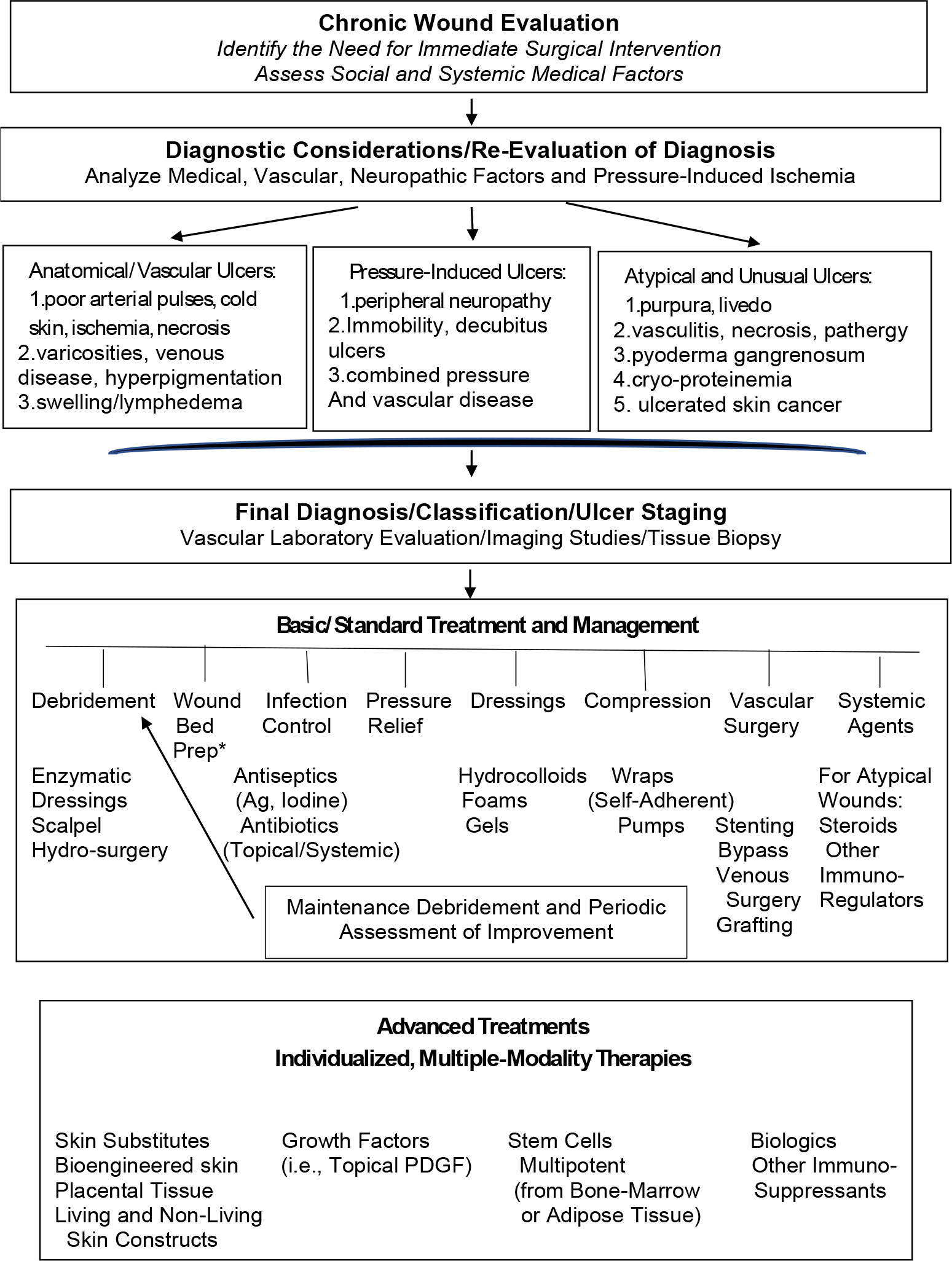
Chronic wounds are characterized by their inability to heal within an expected time frame and have emerged as an increasingly important clinical problem over the past several decades, owing to their increasing incidence and greater recognition of associated morbidity and socio-economic burden. Even up to a few years ago, the management of chronic wounds relied on standards of care that were outdated. However, the approach to these chronic conditions has improved, with better prevention, diagnosis and treatment. Such improvements are due to major advances in understanding of cellular and molecular aspects of basic science, in innovative and technological breakthroughs in treatment modalities from biomedical engineering, and in our ability to conduct well-controlled and reliable clinical research. The evidence-based approaches resulting from these advances have become the new standard of care. At the same time, these improvements are tempered by the recognition that persistent gaps exist in scientific knowledge of impaired healing and the ability of clinicians to reduce morbidity, loss of limb and mortality. Therefore, taking stock of what is known and what is needed to improve understanding of chronic wounds and their associated failure to heal is crucial to ensuring better treatments and outcomes.
© 2022. Springer Nature Limited.
Conflict of interest statement
Competing interests:
The authors declare no competing interests.
Figures

References
-
- Lazarus GS, Cooper DM, Knighton DR, et al. Definitions and guidelines for assessment of wounds and evaluation of healing. Arch Dermatol 1994;130(4):489–93. (https://www.ncbi.nlm.nih.gov/pubmed/8166487). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
