

Second generation androgen receptor antagonists and challenges in prostate cancer treatment
- PMID: 35864113
- PMCID: PMC9304354
- DOI: 10.1038/s41419-022-05084-1
Second generation androgen receptor antagonists and challenges in prostate cancer treatment
Abstract
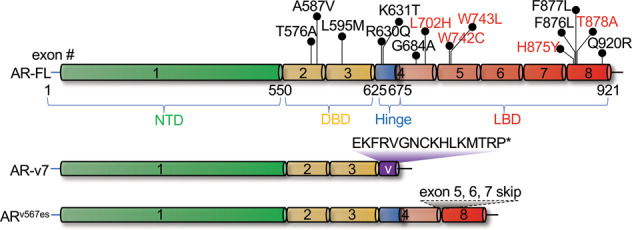
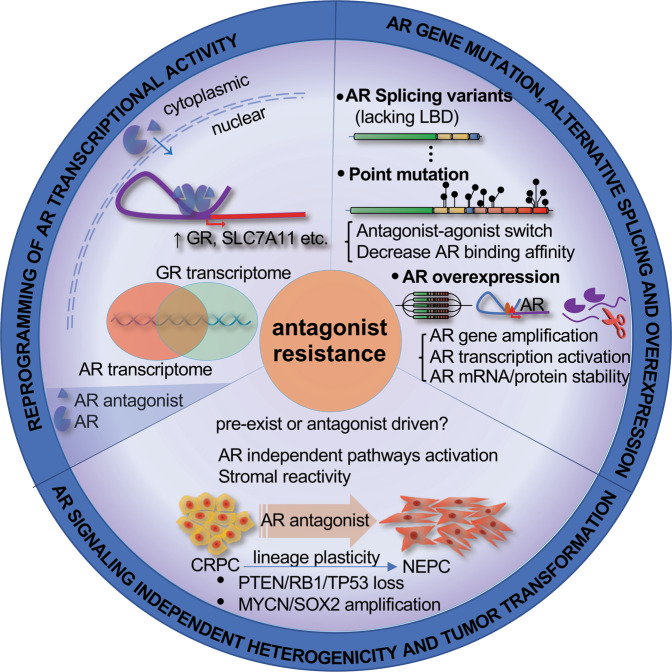
Prostate cancer is a hormone-dependent malignancy, whose onset and progression are closely related to the activity of the androgen receptor (AR) signaling pathway. Due to this critical role of AR signaling in driving prostate cancer, therapy targeting the AR pathway has been the mainstay strategy for metastatic prostate cancer treatment. The utility of these agents has expanded with the emergence of second-generation AR antagonists, which began with the approval of enzalutamide in 2012 by the United States Food and Drug Administration (FDA). Together with apalutamide and darolutamide, which were approved in 2018 and 2019, respectively, these agents have improved the survival of patients with prostate cancer, with applications for both androgen-dependent and castration-resistant disease. While patients receiving these drugs receive a benefit in the form of prolonged survival, they are not cured and ultimately progress to lethal neuroendocrine prostate cancer (NEPC). Here we summarize the current state of AR antagonist development and highlight the emerging challenges of their clinical application and the potential resistance mechanisms, which might be addressed by combination therapies or the development of novel AR-targeted therapies.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71:209–49. - PubMed
-
- Schatzl G, Madersbacher S, Gsur A, Preyer M, Haidinger G, Haitel A, et al. Association of polymorphisms within androgen receptor, 5alpha-reductase, and PSA genes with prostate volume, clinical parameters, and endocrine status in elderly men. Prostate. 2002;52:130–8. doi: 10.1002/pros.10101. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
