

Efficacy and Safety of a Fixed-Dose Combination of Cinnarizine 20 mg and Dimenhydrinate 40 mg in the Treatment of Patients with Vestibular Vertigo: An Individual Patient Data Meta-Analysis of Randomised, Double-Blind, Controlled Clinical Trials
- PMID: 35864302
- PMCID: PMC9427911
- DOI: 10.1007/s40261-022-01184-0
Efficacy and Safety of a Fixed-Dose Combination of Cinnarizine 20 mg and Dimenhydrinate 40 mg in the Treatment of Patients with Vestibular Vertigo: An Individual Patient Data Meta-Analysis of Randomised, Double-Blind, Controlled Clinical Trials
Abstract
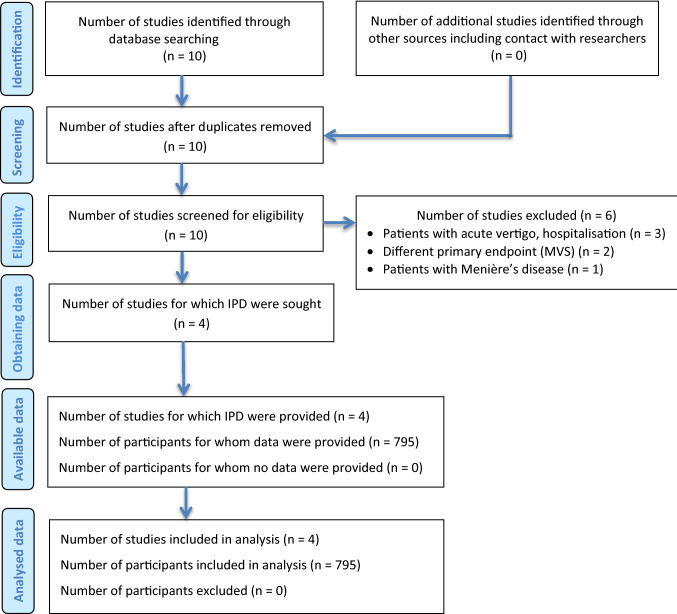
Background and objective: The source data of four individual randomised, double-blind, reference- and/or placebo-controlled clinical trials with virtually identical study design were pooled for the present meta-analysis. The main objective was to further evaluate the efficacy and safety of the fixed combination of cinnarizine 20 mg and dimenhydrinate 40 mg in comparison to various other antivertigo treatments in patients suffering from central and/or peripheral vestibular vertigo.
Methods: Adult male and female outpatients were subjected to a 4-week treatment with the fixed combination of cinnarizine 20 mg and dimenhydrinate 40 mg, cinnarizine (20 mg, 50 mg), dimenhydrinate (40 mg, 100 mg), betahistine dimesylate (12 mg), betahistine dihydrochloride (16 mg) and placebo, respectively. The primary efficacy endpoint was the reduction of a validated mean vertigo score (MVS), a composite score of 12 individual vertigo symptoms, the intensities of which were each evaluated by the patients on a 5-point visual analogue scale. For analysis of primary and further secondary efficacy endpoints, baseline-adjusted analysis of covariance (ANCOVA) was used to calculate adjusted least squares means (LSM) with associated two-sided 95% confidence intervals (CIs) for the difference in MVS reductions between treatment groups. Moreover, various sensitivity analyses, responder and subgroup analyses as well as descriptive analyses with respect to safety/tolerability of the treatments were conducted.
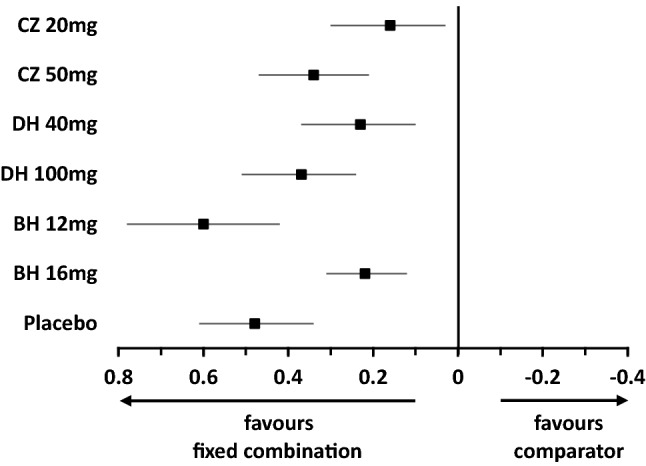
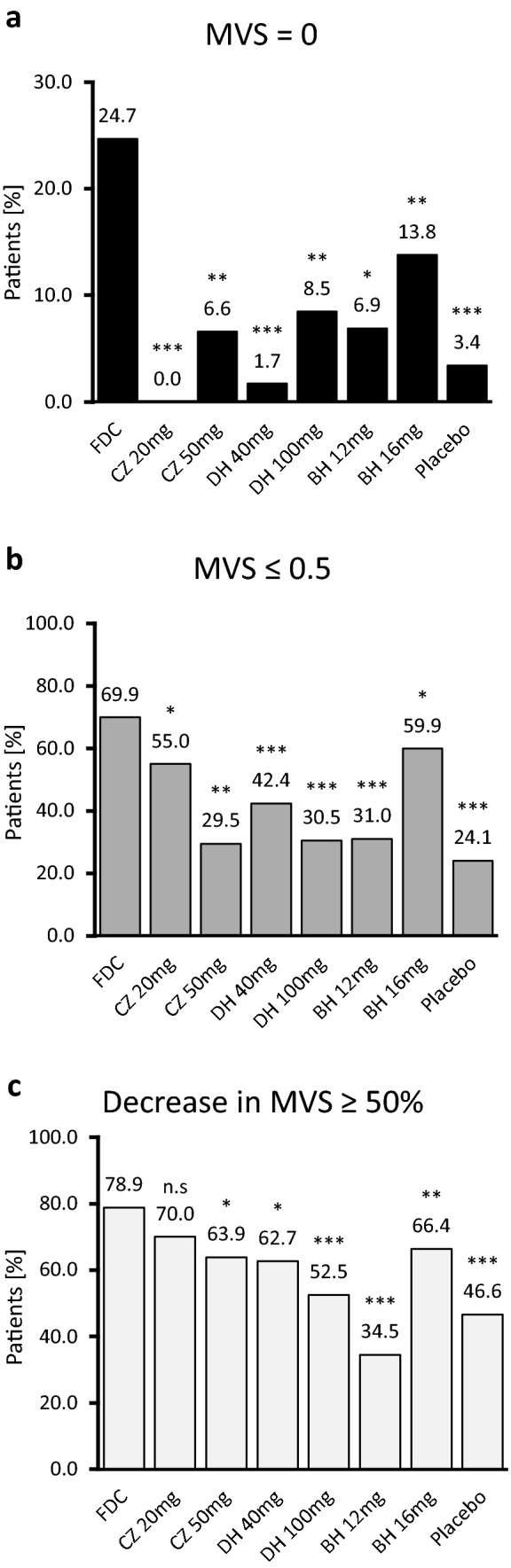
Results: Of 795 randomised patients, 779 belonged to the intent-to treat (ITT) and 723 to the per-protocol (PP) population. The main efficacy analysis was based on the ITT population (mean age 52.1 years, 61% female). The mean decrease of the MVS from baseline to Week 4 in the cinnarizine/dimenhydrinate group (-1.10) proved to be significantly larger than in any of the comparator groups. LSM differences for comparators versus the fixed combination ranged between 0.16 (95% confidence interval (CI) 0.03; 0.30, p = 0.017) for cinnarizine 20 mg and 0.60 (95% CI 0.42; 0.78; p < 0.001) for betahistine dimesylate 12 mg in favour of the fixed combination. Furthermore, after 4 weeks of treatment, 74 patients (24.7%) in the cinnarizine/dimenhydrinate group were completely symptom free (MVS = 0), a significantly greater proportion than in any of the comparator groups. Sensitivity analyses showed that baseline characteristics such as age, sex, duration of vertigo and antivertigo pretreatment had only a very minor and clinically non-relevant impact on the efficacy results regarding the primary efficacy outcome. Subgroup analyses with respect to age groups (< 65 years/≥ 65 years) and sex showed no significant differences in efficacy within any of the treatment groups. All treatments were well tolerated. A total of 55 patients (6.9%) reported 75 non-serious adverse events (AEs), and 19 patients (2.4%) discontinued the study prematurely because of AEs. Nearly 95% of the patients (cinnarizine/dimenhydrinate group: 97.9%) rated the tolerability of the study medications as either "good" or "very good".
Conclusion: The findings of the present meta-analysis indicate that the fixed combination of cinnarizine and dimenhydrinate is a safe and potentially superior treatment option for patients suffering from central and/or peripheral vestibular vertigo, as compared to current standard treatments such as cinnarizine, dimenhydrinate or betahistine given alone in monotherapy.
© 2022. The Author(s).
Conflict of interest statement
Arne W. Scholtz and Frank Waldfahrer have no conflicts of interest that are directly relevant to the content of this article. Regina Hampel is an employee of GKM Gesellschaft für Therapieforschung mbH, Munich, Germany, and Gerhard Weisshaar is an employee of Hennig Arzneimittel.
Figures
References
-
- Schuller DE, Schleuning AJ. DeWeese and Saunders’ Otolaryngology-Head and Neck Surgery. 8. St. Louis: Mosby; 1994. pp. 495–513.
-
- Brandt T, Dieterich M, Strupp M. Vertigo and dizziness—common complaints. 2. London: Springer; 2013.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
