

Accommodating heterogeneous missing data patterns for prostate cancer risk prediction
- PMID: 35864460
- PMCID: PMC9306143
- DOI: 10.1186/s12874-022-01674-x
Accommodating heterogeneous missing data patterns for prostate cancer risk prediction
Abstract
Background: We compared six commonly used logistic regression methods for accommodating missing risk factor data from multiple heterogeneous cohorts, in which some cohorts do not collect some risk factors at all, and developed an online risk prediction tool that accommodates missing risk factors from the end-user.
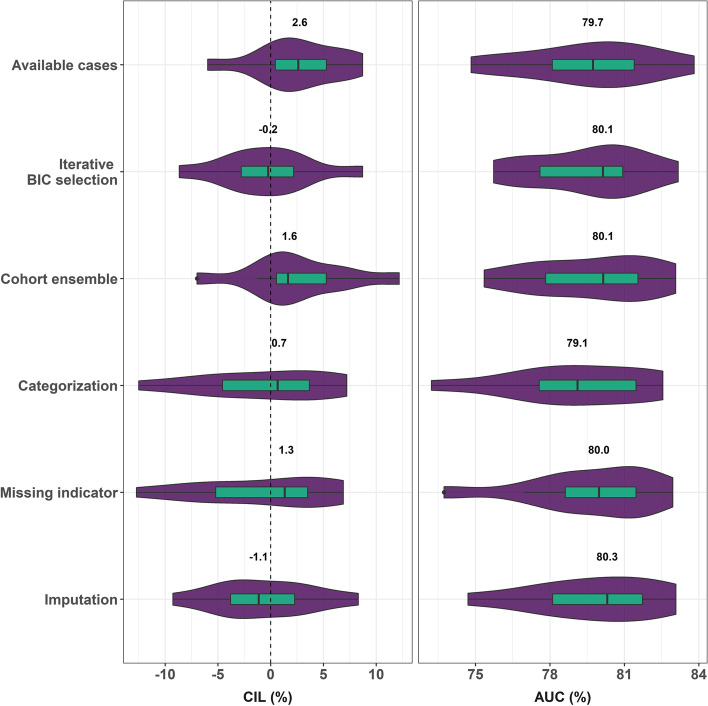
Methods: Ten North American and European cohorts from the Prostate Biopsy Collaborative Group (PBCG) were used for fitting a risk prediction tool for clinically significant prostate cancer, defined as Gleason grade group ≥ 2 on standard TRUS prostate biopsy. One large European PBCG cohort was withheld for external validation, where calibration-in-the-large (CIL), calibration curves, and area-underneath-the-receiver-operating characteristic curve (AUC) were evaluated. Ten-fold leave-one-cohort-internal validation further validated the optimal missing data approach.
Results: Among 12,703 biopsies from 10 training cohorts, 3,597 (28%) had clinically significant prostate cancer, compared to 1,757 of 5,540 (32%) in the external validation cohort. In external validation, the available cases method that pooled individual patient data containing all risk factors input by an end-user had best CIL, under-predicting risks as percentages by 2.9% on average, and obtained an AUC of 75.7%. Imputation had the worst CIL (-13.3%). The available cases method was further validated as optimal in internal cross-validation and thus used for development of an online risk tool. For end-users of the risk tool, two risk factors were mandatory: serum prostate-specific antigen (PSA) and age, and ten were optional: digital rectal exam, prostate volume, prior negative biopsy, 5-alpha-reductase-inhibitor use, prior PSA screen, African ancestry, Hispanic ethnicity, first-degree prostate-, breast-, and second-degree prostate-cancer family history.
Conclusion: Developers of clinical risk prediction tools should optimize use of available data and sources even in the presence of high amounts of missing data and offer options for users with missing risk factors.
Keywords: Clinical risk prediction; Missing data; Prostate cancer; Validation.
© 2022. The Author(s).
Conflict of interest statement
Andrew Vickers receives royalties from the 4Kscore, a test used in prostate cancer. He owns stock options in Opko, which offers the test. All other authors declare that they have no conflict of interest.
Figures




References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
