

Prognostic meaning of right ventricular function and output reserve in patients with systemic sclerosis
- PMID: 35864554
- PMCID: PMC9306074
- DOI: 10.1186/s13075-022-02863-1
Prognostic meaning of right ventricular function and output reserve in patients with systemic sclerosis
Abstract
Background: The objective of this study was to investigate the prognostic impact of right ventricular (RV) function at rest and during exercise in patients with systemic sclerosis (SSc) presenting for a screening for pulmonary hypertension (PH).
Methods: In this study, data from SSc patients who underwent routinely performed examinations for PH screening including echocardiography and right heart catheterization at rest and during exercise were analysed. Uni- and multivariable analyses were performed to identify prognostic parameters.
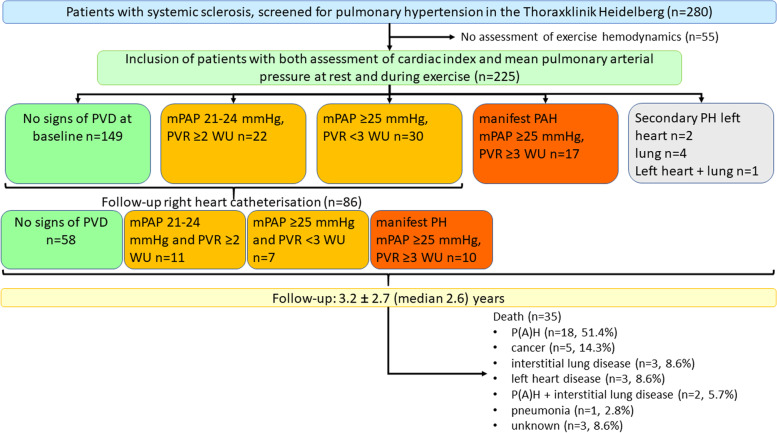
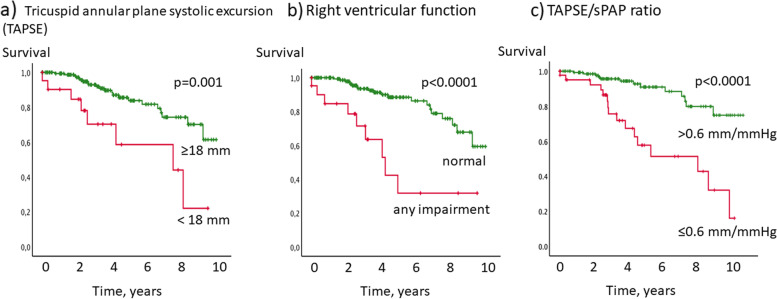
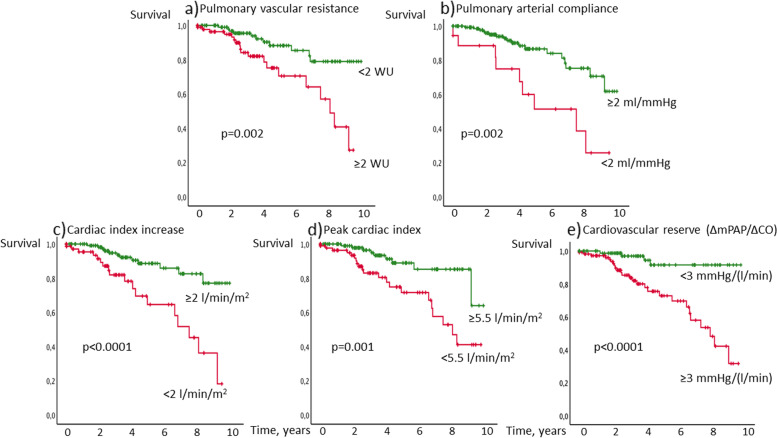
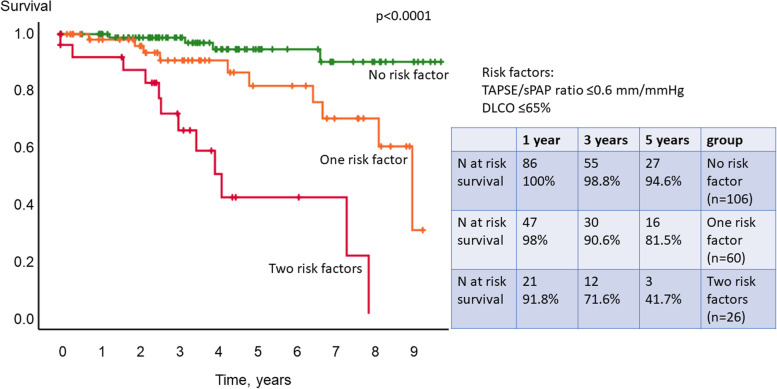
Results: Out of 280 SSc patients screened for PH, 225 were included in the analysis (81.3% female, mean age 58.1±13.0 years, 68% limited cutaneous SSc, WHO-FC II-III 74%, 24 manifest PH). During the observation period of 3.2±2.7 (median 2.6) years 35 patients died. Tricuspid annular plane systolic excursion (TAPSE) at rest <18 mm (p=0.001), RV output reserve as increase of cardiac index (CI) during exercise <2 l/min (p<0.0001), RV pulmonary vascular reserve (Δ mean pulmonary artery pressure/Δ cardiac output) ≥3 mmHg/l/min (p<0.0001), peak CI <5.5 l/min/m2 (p=0.001), pulmonary arterial compliance <2 ml/mmHg (p=0.002), TAPSE/systolic pulmonary arterial pressure (sPAP) ratio ≤0.6 ml/mmHg (p<0.0001) and echocardiographic qualitative RV function at rest (p<0.0001) significantly predicted worse survival. In the multivariable analysis TAPSE/sPAP ratio and diffusion capacity for carbon monoxide ≤65% were identified as independent prognostic predictors and had 75% sensitivity and 69% specificity to predict future development of pulmonary vascular disease (PVD) during follow-up.
Conclusions: This study demonstrates that assessment of RV function at rest and during exercise may provide crucial information to identify SSc patients who are at a high risk of poor outcome and for the development of PH and/or PVD.
Keywords: Echocardiography; Pulmonary hypertension; Right heart catheterisation; Right ventricular reserve; Screening; Systemic sclerosis.
© 2022. The Author(s).
Conflict of interest statement
PX: has received personal fees from MSD and OMT outside the submitted work.
JM, OJ, RS, CAE, NBe: nothing to declare.
BE: received travel fees, consulting fees, speaking fees, and/or honoraria from Actelion, MSD, Bayer and OMT, outside the submitted work.
SH: received honoraria for lectures, consultancy, or both from Actelion, AOP, Bayer/MSD, GSK, Novartis, OMT, Pfizer, and United Therapeutics out-side the submitted work.
AMM: AMM has received personal fees from Bayer, outside the submitted work.
NBl: has received consulting fees, speaking fees and/or honoraria and unallocated funds from Roche out-side the submitted work.
HML: has received consulting fees, speaking fees and/or honoraria and unallocated funds for scientific talks and consultations from Abbvie, Astra-Zeneca, Actelion, Alexion, Amgen, Bayer Vital, Baxter, Biogen, Boehringer Ingelheim, BMS, Celgene, Fresenius, Genzyme, GSK, Gilead/Galapagos, Hexal, Janssen-Cilag, Lilly, Medac, MSD, Mundipharm, Mylan, Novartis, octapharm, Pfizer, Roche/Chugai, Sandoz, Sanofi, Shire, SOBI, Thermo Fisher, UCB.
EG: has received grants and personal fees from Actelion, Bayer AG, and MSD; grants from GSK, Novartis, and United Therapeutics and personal fees from SCOPE, OrPha Swiss GmbH, and Zurich Heart House, outside the submitted work. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures
Similar articles
-
The prognostic role of the echocardiographic tricuspid annular plane systolic excursion/systolic pulmonary arterial pressure (TAPSE/sPAP) ratio and its relationship with NT-proANP plasma level in systemic sclerosis.Front Cardiovasc Med. 2023 Jan 17;9:1021048. doi: 10.3389/fcvm.2022.1021048. eCollection 2022. Front Cardiovasc Med. 2023. PMID: 36733829 Free PMC article.
-
Tricuspid annular plane systolic excursion is a robust outcome measure in systemic sclerosis-associated pulmonary arterial hypertension.J Rheumatol. 2011 Nov;38(11):2410-8. doi: 10.3899/jrheum.110512. Epub 2011 Oct 1. J Rheumatol. 2011. PMID: 21965638
-
Accuracy of Echocardiography to Evaluate Pulmonary Vascular and RV Function During Exercise.JACC Cardiovasc Imaging. 2016 May;9(5):532-43. doi: 10.1016/j.jcmg.2015.06.018. Epub 2015 Oct 21. JACC Cardiovasc Imaging. 2016. PMID: 26508387
-
The role of TAPSE/sPAP ratio in predicting pulmonary hypertension and mortality in the systemic sclerosis EUSTAR cohort.Autoimmun Rev. 2023 Apr;22(4):103290. doi: 10.1016/j.autrev.2023.103290. Epub 2023 Feb 4. Autoimmun Rev. 2023. PMID: 36746368 Review.
-
Expert consensus for performing right heart catheterisation for suspected pulmonary arterial hypertension in systemic sclerosis: a Delphi consensus study with cluster analysis.Ann Rheum Dis. 2014 Jan;73(1):191-7. doi: 10.1136/annrheumdis-2012-202567. Epub 2013 Jan 24. Ann Rheum Dis. 2014. PMID: 23349131
Cited by
-
Effect of ambrisentan in patients with systemic sclerosis and mild pulmonary arterial hypertension: long-term follow-up data from EDITA study.Arthritis Res Ther. 2024 Jul 18;26(1):136. doi: 10.1186/s13075-024-03363-0. Arthritis Res Ther. 2024. PMID: 39026360 Free PMC article. Clinical Trial.
-
Right ventricular function and anemia in heart failure with preserved ejection fraction.Front Cardiovasc Med. 2024 Nov 18;11:1424576. doi: 10.3389/fcvm.2024.1424576. eCollection 2024. Front Cardiovasc Med. 2024. PMID: 39624217 Free PMC article.
-
Combined systolic velocities using tissue Doppler imaging could predict the severity of cirrhosis: a prospective cohort study.Cardiovasc J Afr. 2023 Jul-Aug 23;34(3):175-180. doi: 10.5830/CVJA-2023-034. Epub 2023 Jul 14. Cardiovasc J Afr. 2023. PMID: 37526978 Free PMC article.
-
The right ventricle outflow tract systolic function could predict the severity of the cirrhosis.Turk J Med Sci. 2023 Nov 11;54(1):239-248. doi: 10.55730/1300-0144.5785. eCollection 2024. Turk J Med Sci. 2023. PMID: 38812635 Free PMC article.
-
The predictive role of the TAPSE/sPAP ratio for cardiovascular events and mortality in systemic sclerosis with pulmonary hypertension.Front Cardiovasc Med. 2024 Oct 14;11:1430903. doi: 10.3389/fcvm.2024.1430903. eCollection 2024. Front Cardiovasc Med. 2024. PMID: 39469124 Free PMC article.
References
-
- Mukerjee D, St George D, Coleiro B, Knight C, Denton CP, Davar J, Black CM, Coghlan JG. Prevalence and outcome in systemic sclerosis associated pulmonary arterial hypertension: application of a registry approach. Ann Rheum Dis. 2003;62(11):1088–1093. doi: 10.1136/ard.62.11.1088. - DOI - PMC - PubMed
-
- Wigley FM, Lima JA, Mayes M, McLain D, Chapin JL, Ward-Able C. The prevalence of undiagnosed pulmonary arterial hypertension in subjects with connective tissue disease at the secondary health care level of community-based rheumatologists (the UNCOVER study) Arthritis Rheum. 2005;52(7):2125–2132. doi: 10.1002/art.21131. - DOI - PubMed
-
- Hachulla E, Carpentier P, Gressin V, Diot E, Allanore Y, Sibilia J, Launay D, Mouthon L, Jego P, Cabane J, et al. Risk factors for death and the 3-year survival of patients with systemic sclerosis: the French ItinerAIR-Sclerodermie study. Rheumatology (Oxford) 2009;48(3):304–308. doi: 10.1093/rheumatology/ken488. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
