

Tumor Location May Independently Predict Survival in Patients With M0 Squamous Cell Carcinoma of the Penis
- PMID: 35865480
- PMCID: PMC9294313
- DOI: 10.3389/fonc.2022.927088
Tumor Location May Independently Predict Survival in Patients With M0 Squamous Cell Carcinoma of the Penis
Abstract
Background: To determine the association between tumor location and both clinicopathological characteristics and the survival of patients with M0 squamous cell carcinoma of the penis (SCCP).
Methods: Data of 455 patients diagnosed with M0 SCCP between 1975 and 2018 were collected from the Surveillance, Epidemiology, and End Results (SEER) database of the United States National Cancer Institute. The effects of tumor location on overall survival (OS) and penile carcinoma-specific survival (PCSS) were analyzed using the Kaplan-Meier method. The Cox proportional hazards regression model was used to determine the impact of tumor location on PCSS.
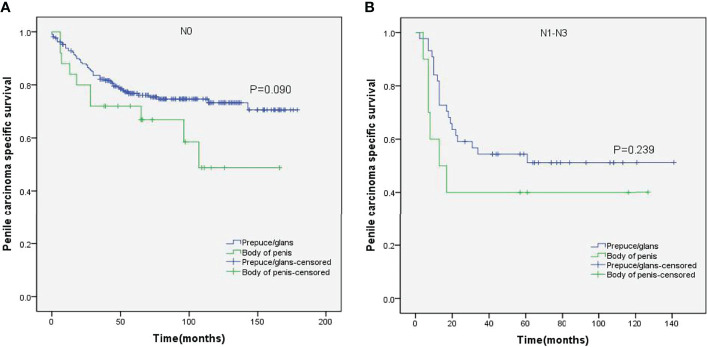
Results: SCCP was more likely to occur in the prepuce or glans (90%). Although no significant difference was observed between the OS of patients with M0 SCCP in the prepuce or glans and those with M0 SCCP in the body of the penis (p = 0.307), the former had better PCSS (p = 0.024). Moreover, M0 SCCP in the prepuce or glans was also significantly associated with better PCSS in patients with advanced age (age ≥ 60 years, p = 0.011), other ethnicities (p = 0.003), T2-T4 stage (p = 0.036), larger tumors (≥3 cm, p = 0.001), no regional lymph nodes removed (p = 0.044), and radical surgery (p = 0.027). Multivariate analysis confirmed that tumor location is an independent prognostic factor for patients with M0 SCCP [hazard ratio (HR) 1.881, p = 0.026].
Conclusions: Tumor location is an independent prognostic factor for patients with M0 SCCP, and tumors in the prepuce or glans portend better PCSS.
Keywords: overall survival; penile carcinoma specific survival; prognostic factor; squamous cell carcinoma of the penis; tumor location.
Copyright © 2022 Li, Le, Wang, Fan and Sun.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures








Similar articles
-
The prognostic significance of primary tumor size in squamous cell carcinoma of the penis.Discov Oncol. 2021 Jul 19;12(1):22. doi: 10.1007/s12672-021-00416-7. Discov Oncol. 2021. PMID: 35201454 Free PMC article.
-
Prognostic value of lymphovascular invasion in patients with squamous cell carcinoma of the penis following surgery.BMC Cancer. 2019 May 21;19(1):476. doi: 10.1186/s12885-019-5714-1. BMC Cancer. 2019. PMID: 31113402 Free PMC article.
-
Ki-67, mini-chromosome maintenance 2 protein (MCM2) and geminin have no independent prognostic relevance for cancer-specific survival in surgically treated squamous cell carcinoma of the penis.BJU Int. 2013 Aug;112(4):E383-90. doi: 10.1111/j.1464-410X.2012.11735.x. Epub 2013 Jan 10. BJU Int. 2013. PMID: 23305250
-
Regional differences in penile cancer patient characteristics and treatment rates across the United States.Cancer Epidemiol. 2023 Oct;86:102424. doi: 10.1016/j.canep.2023.102424. Epub 2023 Jul 26. Cancer Epidemiol. 2023. PMID: 37506474
-
Hepatoid adenocarcinoma of the lung: An analysis of the Surveillance, Epidemiology, and End Results (SEER) database.Open Med (Wars). 2021 Jan 22;16(1):169-174. doi: 10.1515/med-2021-0215. eCollection 2021. Open Med (Wars). 2021. PMID: 33585692 Free PMC article. Review.
Cited by
-
Machine learning-based overall and cancer-specific survival prediction of M0 penile squamous cell carcinoma:A population-based retrospective study.Heliyon. 2023 Dec 8;10(1):e23442. doi: 10.1016/j.heliyon.2023.e23442. eCollection 2024 Jan 15. Heliyon. 2023. PMID: 38163093 Free PMC article.
-
Risk factors for distant metastasis and prognosis of the penile cancer with distant metastasis.Transl Androl Urol. 2024 Jul 31;13(7):1256-1267. doi: 10.21037/tau-24-92. Epub 2024 Jun 11. Transl Androl Urol. 2024. PMID: 39100830 Free PMC article.
References
-
- Ertoy Baydar D, Akkaya H, Dusmez Apa D, Bal N, Demirsam A, Gucluer B, et al. . Squamous Cell Carcinoma of the Penis: A Clinicopathological Study From a Population With Late Circumcision. Rom J Morphol Embryol (2019) 60:521–9. - PubMed
LinkOut - more resources
Full Text Sources