

Three-Dimensional High-Resolution Magnetic Resonance Imaging for the Assessment of Cervical Artery Dissection
- PMID: 35865747
- PMCID: PMC9295408
- DOI: 10.3389/fnagi.2022.785661
Three-Dimensional High-Resolution Magnetic Resonance Imaging for the Assessment of Cervical Artery Dissection
Abstract
Background and purpose: Diagnosing cervical artery dissection (CAD) is still a challenge based on the current radiographic criteria. This study aimed to assess the value of three-dimensional high-resolution magnetic resonance imaging (3D HRMRI) in the detection of the signs of CAD and its diagnosis.
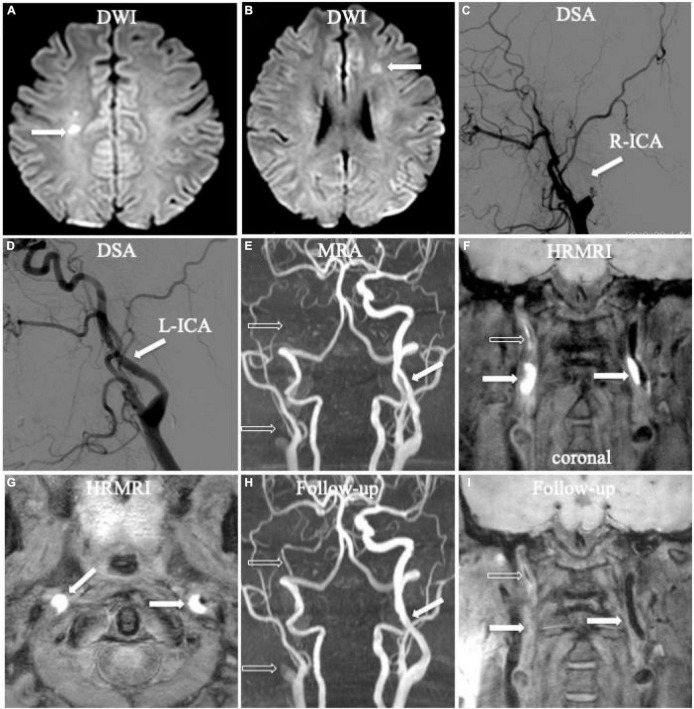
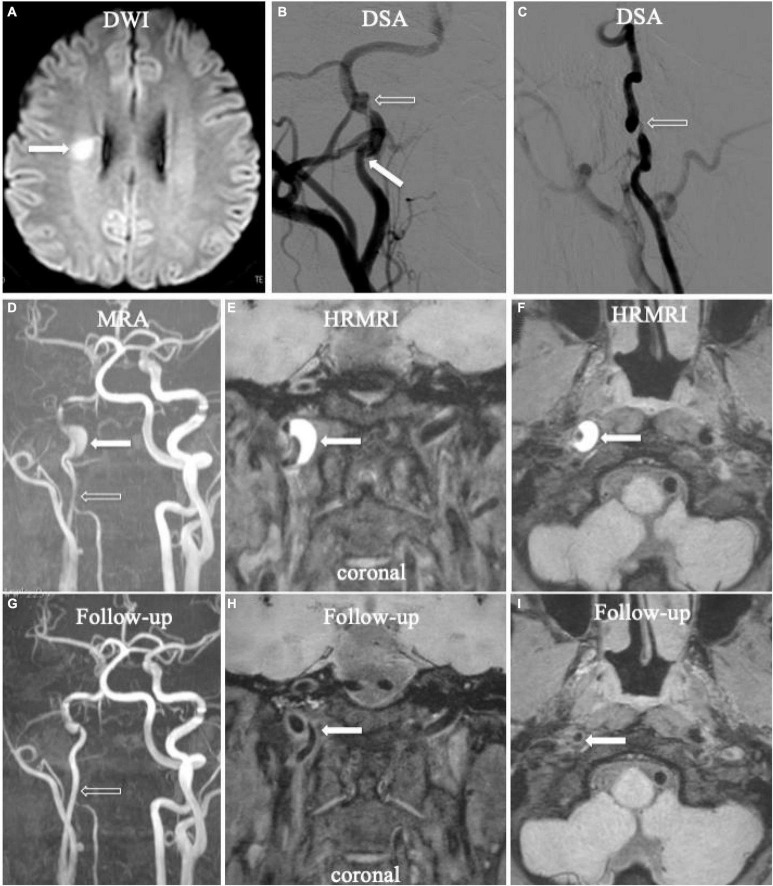
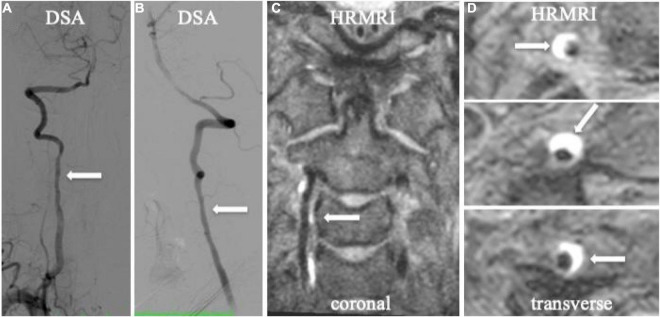
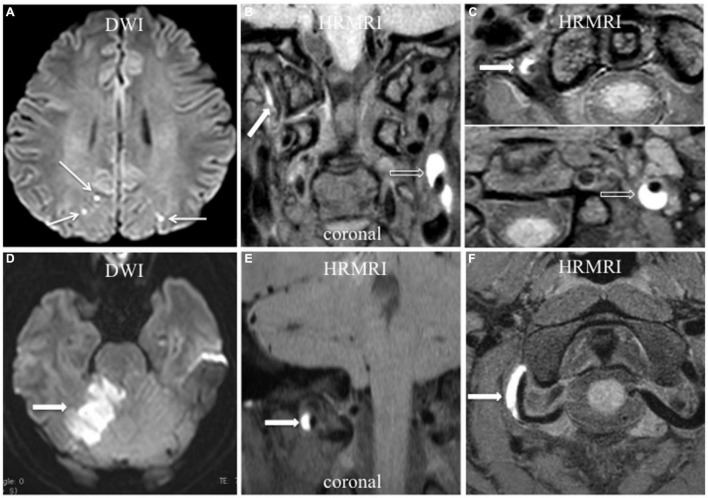
Materials and methods: Patients with CAD from January 2016 to January 2021 were recruited from our 3D HRMRI database. The signs of dissection (intramural hematomas, intimal flap, double lumen), length and location of the dissection, thickness of the intramural hematoma, intraluminal thrombus, and percentage of dilation of the outer contour of the dissection on 3D HRMRI were assessed.
Results: Fourteen patients with 16 CADs, including 12 carotid CADs and 4 vertebral CADs, were finally diagnosed in this study. On 3D HRMRI, intramural hematomas were detected in 13/16 (81.3%) lesions with high sensitivity (100%) and high specificity (100%). Intimal flaps were found in 9/16 (56.3%) lesions with moderate sensitivity (64.3%) and high specificity (88.9%). Double lumen signs were observed in 4/16 (25.0%) lesions with high sensitivity (80.0%) and high specificity (100%). In addition, concomitant intraluminal thrombus were detected in 4/16 (25.0%) lesions with high sensitivity (80.0%) and high specificity (100%). The mean length of dissection was (25.1 ± 13.7) mm. The mean thickness of the intramural hematoma was (4.3 ± 2.3) mm. The mean percentage of dilation for the outer contour of the dissection was (151.3 ± 28.6)%.
Conclusion: The 3D HRMRI enables detection of the dissecting signs, such as intramural hematoma, intimal flap, double lumen, and intraluminal thrombus with high sensitivity and specificity, suggesting a useful, and non-invasive tool for definitively diagnosing CAD.
Keywords: cervical artery dissection; double lumen; high resolution magnetic resonance image; intimal flap; intramural hematoma.
Copyright © 2022 Zhu, Shan, Guo, Zheng, Zhang, Liu and Liu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The reviewer QY declared a shared parent affiliation with the authors, XJZ to the handling editor at the time of review.
Figures
Similar articles
-
Predictors of ischemic events in patients with unilateral extracranial vertebral artery dissection: A single-center exploratory study.Front Neurol. 2022 Jul 28;13:939001. doi: 10.3389/fneur.2022.939001. eCollection 2022. Front Neurol. 2022. PMID: 35968293 Free PMC article.
-
High-resolution magnetic resonance imaging for the follow-up of intracranial arterial dissections.Acta Neurol Belg. 2021 Dec;121(6):1599-1605. doi: 10.1007/s13760-020-01432-0. Epub 2020 Jul 10. Acta Neurol Belg. 2021. PMID: 32651876
-
3D T1-weighted black blood sequence at 3.0 Tesla for the diagnosis of cervical artery dissection.Stroke Vasc Neurol. 2016 Oct 25;1(3):140-146. doi: 10.1136/svn-2016-000028. eCollection 2016 Sep. Stroke Vasc Neurol. 2016. PMID: 28959476 Free PMC article.
-
Imaging of Carotid Dissection.Curr Pain Headache Rep. 2019 Jan 19;23(1):2. doi: 10.1007/s11916-019-0741-9. Curr Pain Headache Rep. 2019. PMID: 30661121 Review.
-
Magnetic resonance imaging, magnetic resonance and catheter angiography for diagnosis of cervical artery dissection.Front Neurol Neurosci. 2005;20:102-118. doi: 10.1159/000088155. Front Neurol Neurosci. 2005. PMID: 17290116 Review.
Cited by
-
Studying the imaging features and infarction mechanism of vertebrobasilar dolichoectasia with high-resolution magnetic resonance imaging.Brain Pathol. 2023 Mar;33(2):e13135. doi: 10.1111/bpa.13135. Epub 2023 Jan 31. Brain Pathol. 2023. PMID: 36718993 Free PMC article.
-
Post-Traumatic Cerebral Infarction: A Narrative Review of Pathophysiology, Diagnosis, and Treatment.Neurol Int. 2024 Jan 4;16(1):95-112. doi: 10.3390/neurolint16010006. Neurol Int. 2024. PMID: 38251054 Free PMC article. Review.
-
Enhancing intracranial aneurysm rupture risk prediction with a novel multivariable logistic regression model incorporating high-resolution vessel wall imaging.Front Neurol. 2025 Jan 7;15:1507082. doi: 10.3389/fneur.2024.1507082. eCollection 2024. Front Neurol. 2025. PMID: 39944838 Free PMC article.
-
Beyond the "string of beads": case-based exploration of diagnostic pitfalls and solutions in reversible cerebral vasoconstriction syndrome.J Headache Pain. 2025 Apr 28;26(1):89. doi: 10.1186/s10194-025-01978-5. J Headache Pain. 2025. PMID: 40289076 Free PMC article. Review.
-
[Reconstruction of internal carotid artery in the resection of paraganglioma of head and neck].Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2024 Sep;38(9):802-807;811. doi: 10.13201/j.issn.2096-7993.2024.09.005. Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2024. PMID: 39193736 Free PMC article. Chinese.
References
-
- Bachmann R., Nassenstein I., Kooijman H., Dittrich R., Stehling C., Kugel H., et al. (2007). High-resolution magnetic resonance imaging (MRI) at 3.0 tesla in the short-term follow-up of patients with proven cervical artery dissection. Invest. Radiol. 42 460–466. 10.1097/01.rli.0000262758.98098.d6 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous