

Sero-prevalence and risk factors for Severe Acute Respiratory Syndrome Coronavirus 2 infection in women and children in a rural district of Bangladesh: A cohort study
- PMID: 35866222
- PMCID: PMC9304923
- DOI: 10.7189/jogh.12.05030
Sero-prevalence and risk factors for Severe Acute Respiratory Syndrome Coronavirus 2 infection in women and children in a rural district of Bangladesh: A cohort study
Abstract
Background: Bangladesh reported its first COVID-19 case on March 8, 2020. Despite lockdowns and promoting behavioural interventions, as of December 31, 2021, Bangladesh reported 1.5 million confirmed cases and 27 904 COVID-19-related deaths. To understand the course of the pandemic and identify risk factors for SARs-Cov-2 infection, we conducted a cohort study from November 2020 to December 2021 in rural Bangladesh.
Methods: After obtaining informed consent and collecting baseline data on COVID-19 knowledge, comorbidities, socioeconomic status, and lifestyle, we collected data on COVID-like illness and care-seeking weekly for 54 weeks for women (n = 2683) and their children (n = 2433). Between March and July 2021, we tested all participants for SARS-CoV-2 antibodies using ROCHE's Elecsys® test kit. We calculated seropositivity rates and 95% confidence intervals (95% CI) separately for women and children. In addition, we calculated unadjusted and adjusted relative risk (RR) and 95% CI of seropositivity for different age and risk groups using log-binomial regression models.
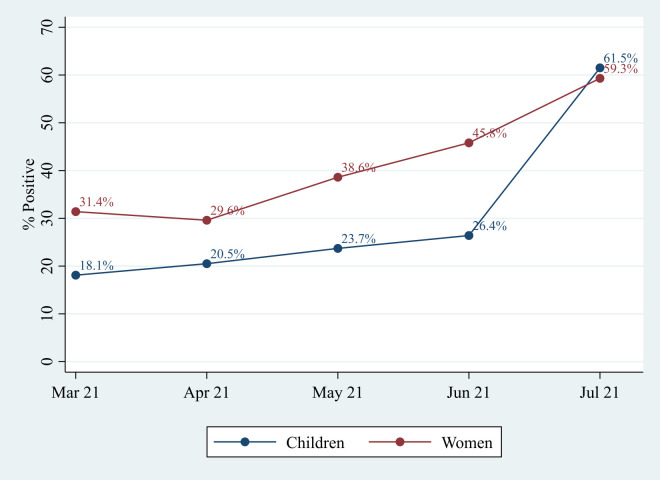
Results: Overall, about one-third of women (35.8%, 95% CI = 33.7-37.9) and one-fifth of children (21.3%, 95% CI = 19.2-23.6) were seropositive for SARS-CoV-2 antibodies. The seroprevalence rate doubled for women and tripled for children between March 2021 and July 2021. Compared to women and children with the highest household wealth (HHW) tertile, both women and children from poorer households had a lower risk of infection (RR, 95% CI for lowest HHW tertile women (0.83 (0.71-0.97)) and children (0.75 (0.57-0.98)). Most infections were asymptomatic or mild. In addition, the risk of infection among women was higher if she reported chewing tobacco (RR = 1.19,95% CI = 1.03-1.38) and if her husband had an occupation requiring him to work indoors (RR = 1.16, 95% CI = 1.02-1.32). The risk of infection was higher among children if paternal education was >5 years (RR = 1.37, 95% CI = 1.10-1.71) than in children with a paternal education of ≤5 years.
Conclusions: We provided prospectively collected population-based data, which could contribute to designing feasible strategies against COVID-19 tailored to high-risk groups. The most feasible strategy may be promoting preventive care practices; however, collecting data on reported practices is inadequate. More in-depth understanding of the factors related to adoption and adherence to the practices is essential.
Copyright © 2022 by the Journal of Global Health. All rights reserved.
Conflict of interest statement
Disclosure of interest: The authors completed the ICMJE Unified Competing Interest form (available upon request from the corresponding author) and declare no conflicts of interest.
Figures
References
-
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available: https://covid19.who.int/. Accessed: January 2 2022. 2022.
-
- World Health Organization. Considerations for implementing and adjusting public health and social measures in the context of COVID-19: interim guidance, June 14 2021. World Health Organization. Available: https://apps.who.int/iris/handle/10665/341811. Accessed: January 19 2022.
-
- Centers for Disease Control and Prevention. Coronavirus Disease 2019 - How to Protect Yourself & Others. Available: https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/social-di.... Accessed: January 19 2022.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
