

Single-cell immune profiling reveals long-term changes in myeloid cells and identifies a novel subset of CD9+ monocytes associated with COVID-19 hospitalization
- PMID: 35866369
- PMCID: PMC9350203
- DOI: 10.1002/JLB.4COVA0122-076R
Single-cell immune profiling reveals long-term changes in myeloid cells and identifies a novel subset of CD9+ monocytes associated with COVID-19 hospitalization
Abstract
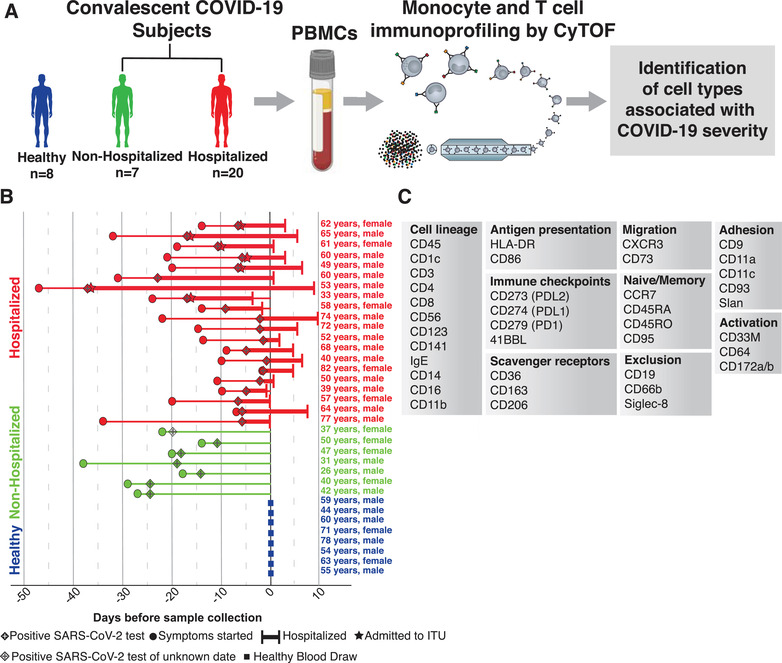
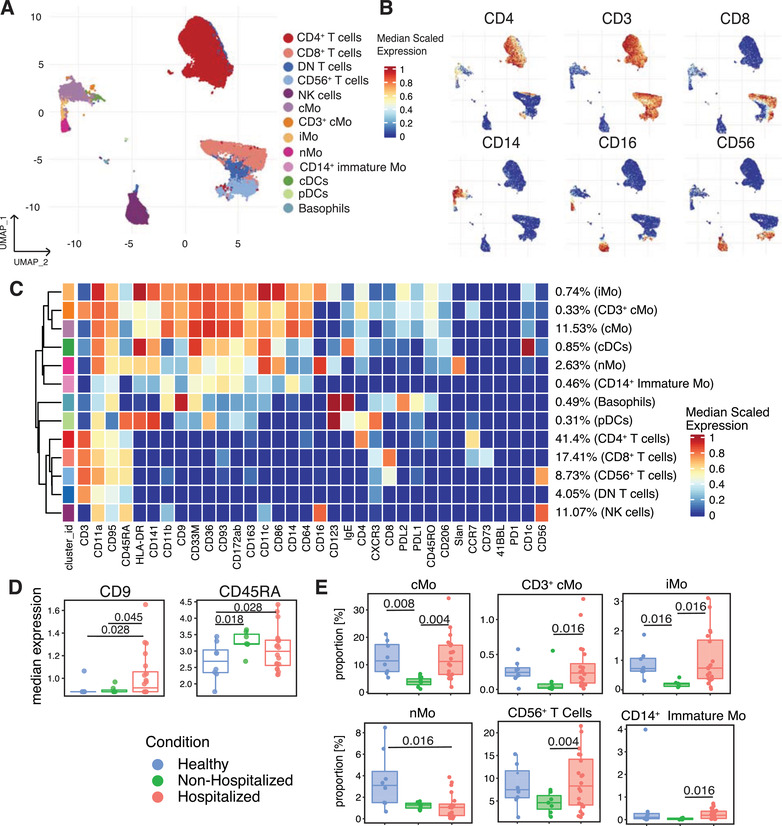
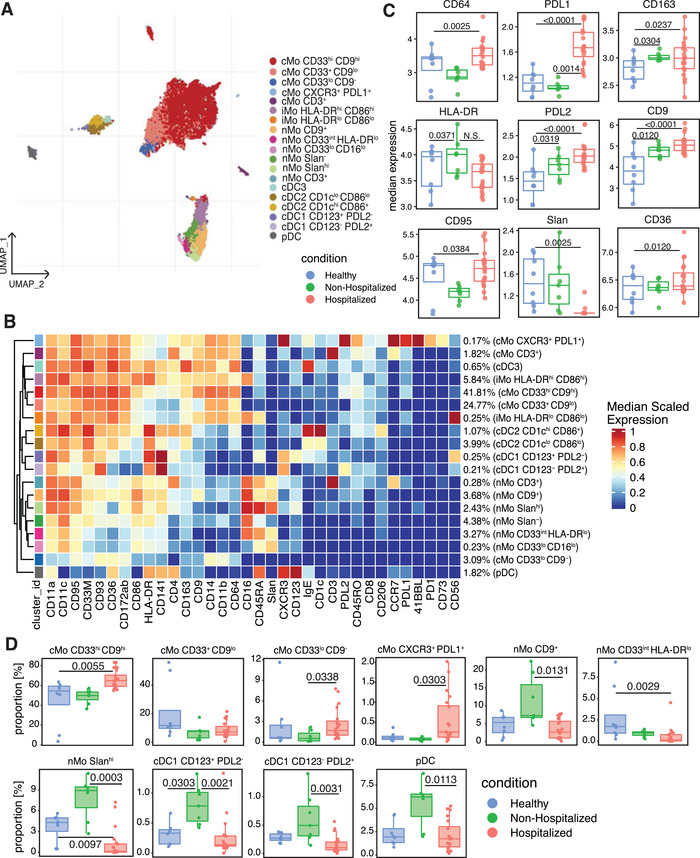
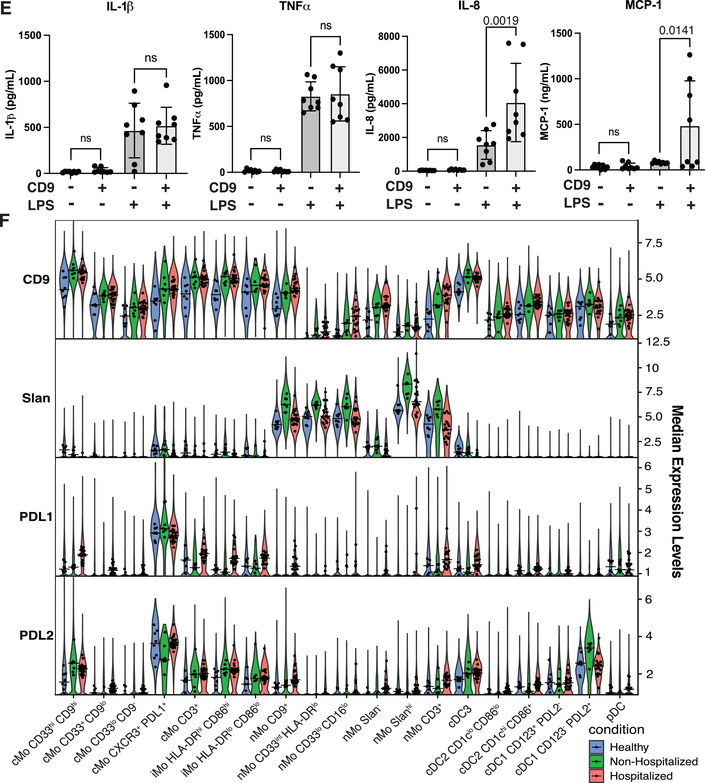
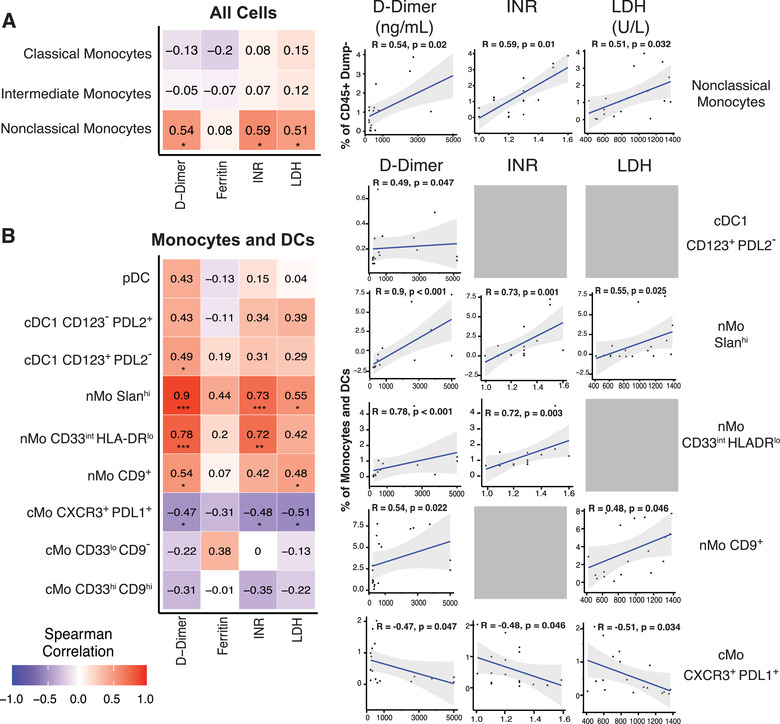
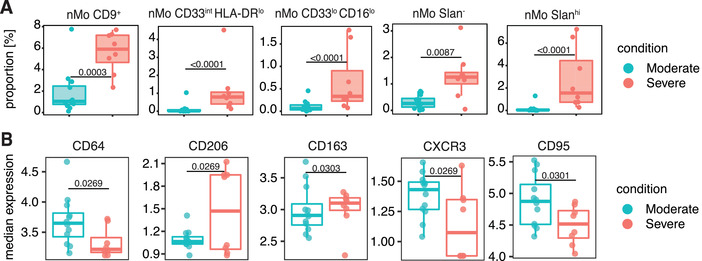
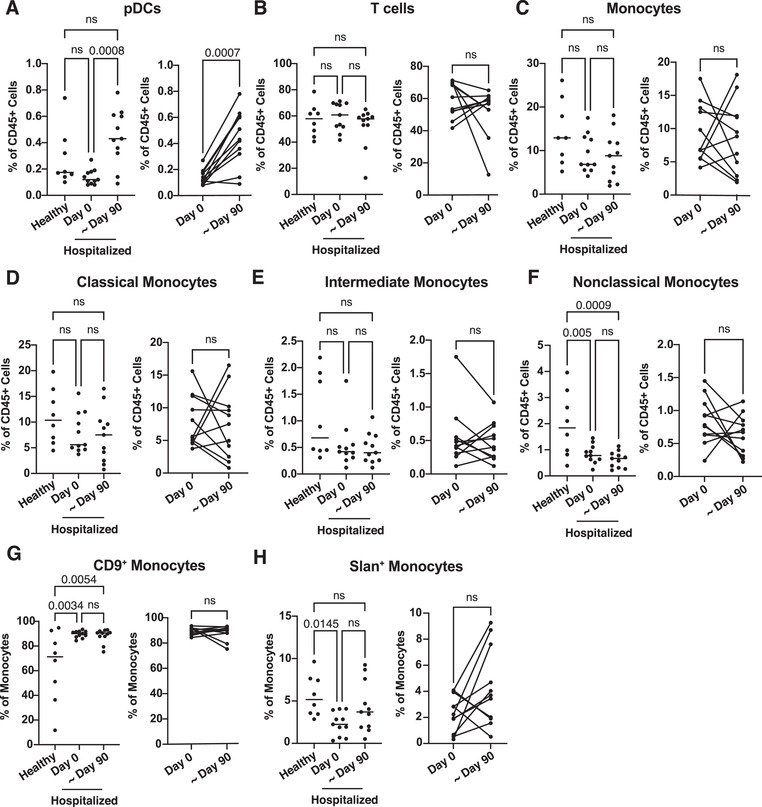
Coronavirus disease 2019 (COVID-19) caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection can result in severe immune dysfunction, hospitalization, and death. Many patients also develop long-COVID-19, experiencing symptoms months after infection. Although significant progress has been made in understanding the immune response to acute SARS-CoV-2 infection, gaps remain in our knowledge of how innate immunity influences disease kinetics and severity. We hypothesized that cytometry by time-of-flight analysis of PBMCs from healthy and infected subjects would identify novel cell surface markers and innate immune cell subsets associated with COVID-19 severity. In this pursuit, we identified monocyte and dendritic cell subsets that changed in frequency during acute SARS-CoV-2 infection and correlated with clinical parameters of disease severity. Subsets of nonclassical monocytes decreased in frequency in hospitalized subjects, yet increased in the most severe patients and positively correlated with clinical values associated with worse disease severity. CD9, CD163, PDL1, and PDL2 expression significantly increased in hospitalized subjects, and CD9 and 6-Sulfo LacNac emerged as the markers that best distinguished monocyte subsets amongst all subjects. CD9+ monocytes remained elevated, whereas nonclassical monocytes remained decreased, in the blood of hospitalized subjects at 3-4 months postinfection. Finally, we found that CD9+ monocytes functionally released more IL-8 and MCP-1 after LPS stimulation. This study identifies new monocyte subsets present in the blood of COVID-19 patients that correlate with disease severity, and links CD9+ monocytes to COVID-19 progression.
Keywords: CyTOF; SARS-CoV-2; Slan; T cells; long-COVID-19; nonclassical monocytes.
©2022 Society for Leukocyte Biology.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Major alterations to monocyte and dendritic cell subsets lasting more than 6 months after hospitalization for COVID-19.Front Immunol. 2023 Jan 4;13:1082912. doi: 10.3389/fimmu.2022.1082912. eCollection 2022. Front Immunol. 2023. PMID: 36685582 Free PMC article.
-
Reduced monocyte proportions and responsiveness in convalescent COVID-19 patients.Front Immunol. 2024 Jan 4;14:1329026. doi: 10.3389/fimmu.2023.1329026. eCollection 2023. Front Immunol. 2024. PMID: 38250080 Free PMC article.
-
Severe COVID-19 Recovery Is Associated with Timely Acquisition of a Myeloid Cell Immune-Regulatory Phenotype.Front Immunol. 2021 Jun 23;12:691725. doi: 10.3389/fimmu.2021.691725. eCollection 2021. Front Immunol. 2021. PMID: 34248984 Free PMC article.
-
Tetraspanin-enriched Microdomain Containing CD151, CD9, and TSPAN 8 - Potential Mediators of Entry and Exit Mechanisms in Respiratory Viruses Including SARS-CoV-2.Curr Pharm Des. 2022;28(46):3649-3657. doi: 10.2174/1381612828666220907105543. Curr Pharm Des. 2022. PMID: 36173052 Review.
-
Dysregulated Immune Responses in SARS-CoV-2-Infected Patients: A Comprehensive Overview.Viruses. 2022 May 18;14(5):1082. doi: 10.3390/v14051082. Viruses. 2022. PMID: 35632823 Free PMC article. Review.
Cited by
-
Correlations of Long COVID Symptoms and Inflammatory Markers of Complete Blood Count (CBC): A Cross-sectional Study.J Community Hosp Intern Med Perspect. 2023 Nov 4;13(6):112-119. doi: 10.55729/2000-9666.1259. eCollection 2023. J Community Hosp Intern Med Perspect. 2023. PMID: 38596549 Free PMC article.
-
Immunomodulatory Mechanisms Underlying Neurological Manifestations in Long COVID: Implications for Immune-Mediated Neurodegeneration.Int J Mol Sci. 2025 Jun 27;26(13):6214. doi: 10.3390/ijms26136214. Int J Mol Sci. 2025. PMID: 40649991 Free PMC article. Review.
-
Mechanisms of long COVID: An updated review.Chin Med J Pulm Crit Care Med. 2023 Dec 6;1(4):231-240. doi: 10.1016/j.pccm.2023.10.003. eCollection 2023 Dec. Chin Med J Pulm Crit Care Med. 2023. PMID: 39171285 Free PMC article. Review.
-
The role of trained immunity in COVID-19: Lessons for the next pandemic.Cell Host Microbe. 2023 Jun 14;31(6):890-901. doi: 10.1016/j.chom.2023.05.004. Cell Host Microbe. 2023. PMID: 37321172 Free PMC article. Review.
-
Patients Hospitalized with COVID-19 Demonstrate Distinct Plasma Cytokine and Chemokine Concentrations in vivo and TLR-Mediated Cytokine and Chemokine Production in Whole Blood in vitro.J Innate Immun. 2025;17(1):288-301. doi: 10.1159/000545432. Epub 2025 May 28. J Innate Immun. 2025. PMID: 40435967 Free PMC article.
References
-
- Laing AG, Lorenc A, del Molino del Barrio I, et al. A dynamic COVID‐19 immune signature includes associations with poor prognosis. Nat Med. 2020;26:1623‐1635. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
