

Aortic arch plaque morphology in patients with coronary artery disease undergoing coronary computed tomography angiography with wide-volume scan
- PMID: 35866499
- PMCID: PMC9528935
- DOI: 10.1097/MCA.0000000000001171
Aortic arch plaque morphology in patients with coronary artery disease undergoing coronary computed tomography angiography with wide-volume scan
Abstract
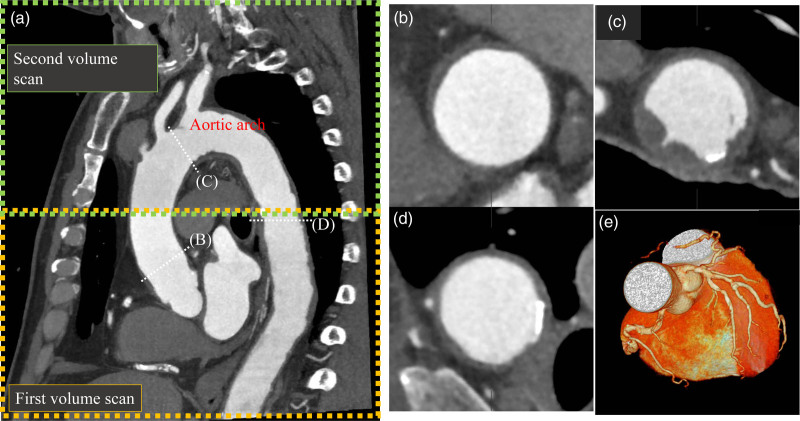
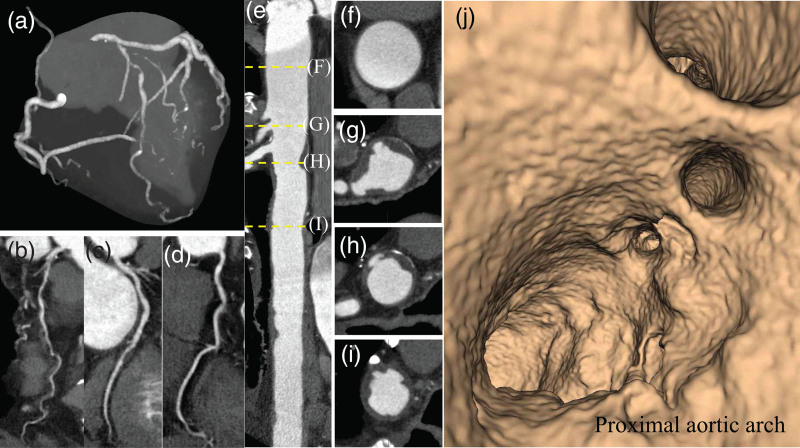
Background: Wide-volume scanning with 320-row multidetector computed tomography coronary angiography (CTCA-WVS) enables the assessment of the aortic arch plaque (AAP) morphology and coronary arteries without requiring additional contrast volume. This study aimed to investigate the prevalence of AAPs and their association with coronary artery disease (CAD) and major adverse cardiovascular events (MACEs) in patients who underwent CTCA-WVS.
Methods: This study included 204 patients without known CAD (mean age, 65 years; 53% men) who underwent CTCA-WVS. We evaluated the presence of aortic plaques in the ascending aorta, aortic arch, and thoracic descending aorta using CTCA-WVS. Large aortic plaques were defined as plaques of at least 4 mm in thickness. A complex aortic plaque was defined as a plaque with ulceration or protrusion. MACEs were defined as composite events of cardiovascular (CV) death, nonfatal myocardial infarction, and ischemic stroke.
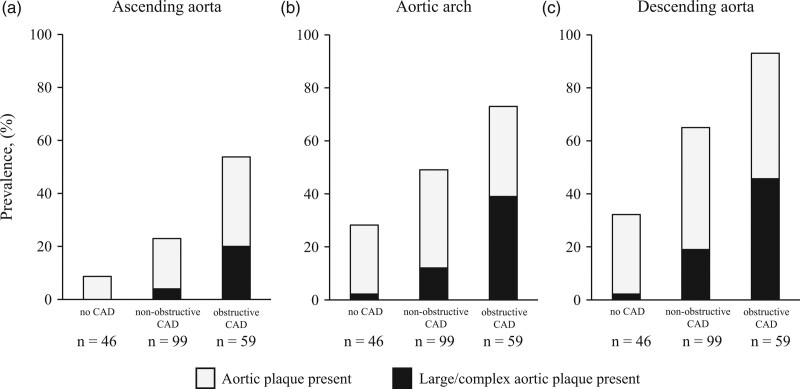
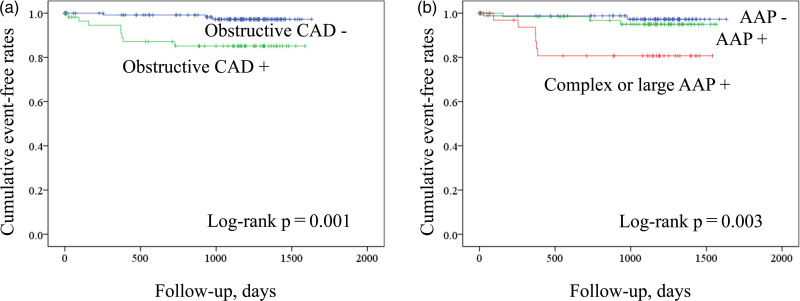
Results: AAPs and large/complex AAPs were identified in 51% ( n = 105) and 18% ( n = 36) of the study patients, respectively. The prevalence of AAPs with large/complex morphology increased with CAD severity (2.1% in no CAD, 12% in nonobstructive CAD, and 39% in obstructive CAD). The univariate Cox hazard model demonstrated that the predictors associated with MACEs were diabetes, obstructive CAD, and large/complex AAPs. Independent factors associated with large/complex AAPs were male sex [odds ratio (OR), 2.90; P = 0.025], stroke history (OR, 3.48; P = 0.026), obstructive CAD (OR, 3.35; P = 0.011), and thoracic aortic calcification (OR, 1.77; P = 0.005).
Conclusion: CTCA-WVS provides a comprehensive assessment of coronary atherosclerosis and thoracic aortic plaques in patients with CAD, which may improve the stratification of patients at risk for CV events.
Copyright © 2022 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Kernan WN, Ovbiagele B, Black HR, Bravata DM, Chimowitz MI, Ezekowitz MD, et al. ; American Heart Association Stroke Council, Council on Cardiovascular and Stroke Nursing, Council on Clinical Cardiology, and Council on Peripheral Vascular Disease. Guidelines for the prevention of stroke in patients with stroke and transient ischemic attack: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2014; 45:2160–2236. - PubMed
-
- Benjamin EJ, Muntner P, Alonso A, Bittencourt MS, Callaway CW, Carson AP, et al. ; American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics-2019 update: a report from the American Heart Association. Circulation. 2019; 139:e56–e528. - PubMed
-
- Matsumura Y, Sugioka K, Fujita S, Ito A, Iwata S, Yoshiyama M. Association between chronic kidney disease and thoracic aortic atherosclerosis detected using transesophageal echocardiography. Atherosclerosis. 2014; 237:301–306. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
