

Emergency department personnel patient care-related COVID-19 risk
- PMID: 35867681
- PMCID: PMC9307202
- DOI: 10.1371/journal.pone.0271597
Emergency department personnel patient care-related COVID-19 risk
Abstract
Objectives: Emergency department (ED) health care personnel (HCP) are at risk of exposure to SARS-CoV-2. The objective of this study was to determine the attributable risk of SARS-CoV-2 infection from providing ED care, describe personal protective equipment use, and identify modifiable ED risk factors. We hypothesized that providing ED patient care increases the probability of acquiring SARS-CoV-2 infection.
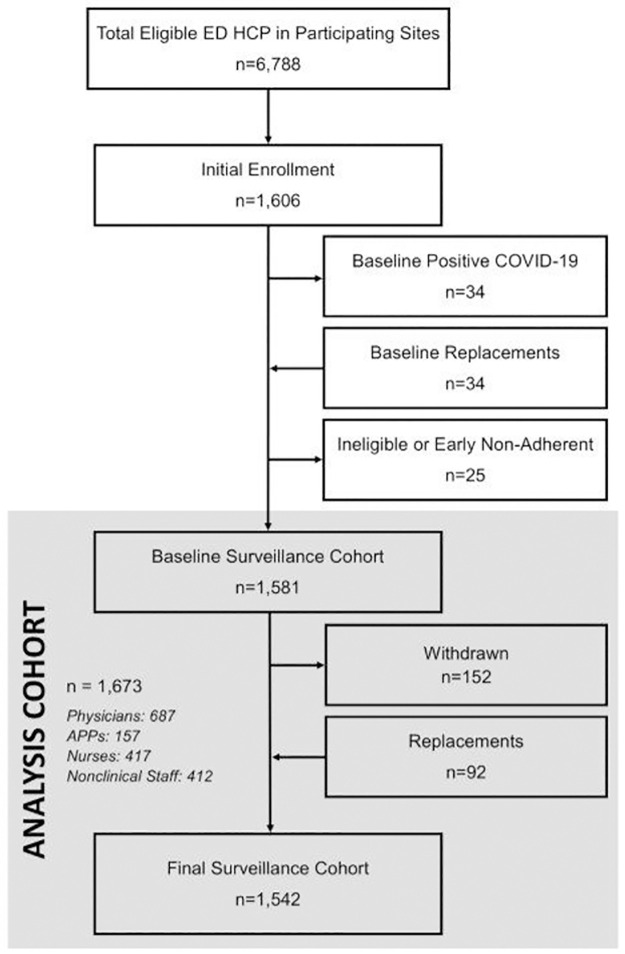
Methods: We conducted a multicenter prospective cohort study of 1,673 ED physicians, advanced practice providers (APPs), nurses, and nonclinical staff at 20 U.S. centers over 20 weeks (May to December 2020; before vaccine availability) to detect a four-percentage point increased SARS-CoV-2 incidence among HCP related to direct patient care. Participants provided monthly nasal and serology specimens and weekly exposure and procedure information. We used multivariable regression and recursive partitioning to identify risk factors.
Results: Over 29,825 person-weeks, 75 participants (4.5%) acquired SARS-CoV-2 infection (31 were asymptomatic). Physicians/APPs (aOR 1.07; 95% CI 0.56-2.03) did not have higher risk of becoming infected compared to nonclinical staff, but nurses had a marginally increased risk (aOR 1.91; 95% CI 0.99-3.68). Over 99% of participants used CDC-recommended personal protective equipment (PPE), but PPE lapses occurred in 22.1% of person-weeks and 32.1% of SARS-CoV-2-infected patient intubations. The following factors were associated with infection: household SARS-CoV-2 exposure; hospital and community SARS-CoV-2 burden; community exposure; and mask non-use in public. SARS-CoV-2 intubation was not associated with infection (attributable risk fraction 13.8%; 95% CI -2.0-38.2%), and nor were PPE lapses.
Conclusions: Among unvaccinated U.S. ED HCP during the height of the pandemic, the risk of SARS-CoV-2 infection was similar in nonclinical staff and HCP engaged in direct patient care. Many identified risk factors were related to community exposures.
Conflict of interest statement
The authors have declared no competing interests exist.
Figures


References
-
- Ghebreyesus T. Director-General’s opening remarks at the World Health Assembly [24 May 2021] 2021 [https://www.who.int/director-general/speeches/detail/director-general-s-....
-
- Mazumdar T. Covid: Global healthcare workers missing out on jabs: BBC News; 18 Jul 2021 [https://www.bbc.com/news/health-57820346.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
